Support WBUR
Commentary
'Faith Healing' And Chest Pain: Heart Controversy Points Up Confounding Power Of Reassurance

Say you, like 16 million Americans, have "stable angina" -- a type of squeezing or burning chest pain that comes on with exercise or stress, and goes away with rest or if you take medications called nitrates.
Understandably, your chest pain worries you, so you see your doctor or a cardiologist, who does some tests and confidently tells you that, while you have heart disease, it isn’t severe enough to require surgery or another invasive procedure called a stent. You’re on the right medications, you're told, and you don’t need to worry.
That’s a good feeling, not needing to worry.
But that reassurance is at the center of a big controversy roiling the cardiology world right now, over how to treat angina patients like you.
The wrangling involves a recent high-quality study that shocked the medical world by showing that stents do not seem to help people with stable angina. At stake is the treatment for millions of patients, hundreds of thousands of procedures each year and billions of dollars of medical care.
Definitive research is urgently needed on when to stent, and a major study with that goal is underway. But a recent cardiology journal commentary warns that the study might end up too biased to finally resolve the issue.
'Faith Healing,' But Not The Religious Kind
Here is where the effects of reassurance come in, or what the commentary calls "faith healing" -- though it isn't referring to the religious miracle type.
Rather, certain heart studies reveal an interesting phenomenon: It seems that if patients are confidently told that they don’t need a procedure, they feel measurably better.
Or as I would put it: Holy cow, sometimes chest pain seems to be cured by reassuring patients they have nothing to worry about!
To be clear, this “faith healing” doesn't imply that words alone cure heart disease. But when doctors and patients know that a procedure is unnecessary, some placebo-like effect seems to be helping patients experience less chest pain.
To understand why this is important, let's look at why all these cardiologists are jabbing at each other.
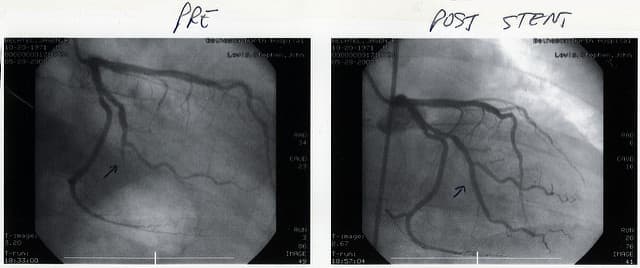
When someone is having a heart attack, the evidence is clear that cardiologists should perform a procedure called a catheterization to see the heart's arteries. Once they find a blockage, they place a stent -- which looks like a tiny, wire version of a bamboo finger trap — to open it up. You can watch this with X-ray in real-time and see the dramatic changes in blood flow around the heart as an invisible artery suddenly becomes visible.
But for patients who have stable angina rather than heart attacks, cardiologists have been debating for ages whether they should get stents or not.
Common Sense
It seems like common sense: If the angina pain is caused by narrowed arteries, opening them up should reduce the pain.
But a landmark 2007 trial showed that giving angina patients a stent does not significantly reduce the risk of death or heart attack. Other studies have come out with conflicting results.
Why doesn't common sense seem to be working? Doctors think that though we can see visible blockages in a big artery, it might be microscopic blockages that are actually causing the pain. Opening the big artery won’t fix the many small ones that are probably at least partially blocked too.
That recent high-quality study, called ORBITA, had extraordinary power as the first-ever blinded, placebo-controlled study of stents in stable angina. (“Blinded” in this case means researchers catheterized all patients with stable angina but neither patients nor their doctors knew who got stents and who didn’t.)
The study was tiny — only about 200 people — but it surprised doctors worldwide by showing that there was no difference in results between those who got stents and those who didn't. It seemed to spell the end for treating stable angina with stents.
The Next Big Study
But cardiologists still stent about 500,000 stable angina patients worldwide each year. So researchers designed a new study, called ISCHEMIA, to finally, definitively, answer the burning question of: to stent or not to stent. It hasn't yet been published but it's already mired in controversy.
In it, not everyone gets catheterized, so it can't be blinded. But unlike previous inconclusive studies, researchers planned to focus only on "hard" outcomes, like deaths and heart attacks, that don't rely on judgment calls. That would leave out squishier measures, like assessments of pain or the decision to admit someone to the hospital.
But at the last minute, the commentary says, the study designers decided to include the measures that involve judgment calls. (The ISCHEMIA researchers claim this is false, and the squishier endpoints were a possibility from the beginning.)
This may seem like small potatoes, but it's a big deal. Researchers like to measure black-and-white outcomes that are clear and objective. But judgment calls are often gray areas susceptible to bias. And the more bias a trial has, the harder it is to trust it. So there's concern that ISCHEMIA will leave us without a conclusive answer.
Here's where the “faith healing” comes in: The commentary authors suggest ISCHEMIA may not answer the big question because of this mysterious "faith healing" effect. They use two famous cardiology studies — called DEFER and FAME 2 -- as reminders of what happens in unblinded trials with lots of judgment calls.
In both studies, doctors and patients both knew how bad (or not) the blockages were. And in both studies, one group of patients whose doctors made clear their heart disease was not severe saw their chest pain decrease or disappear. "This simple act of the telling," as the commentary put it, made the difference.
And this is the risk for the ISCHEMIA trial: That without blinding whether people get stents or not, plus the squishier outcomes, there is the potential for reassurance and "faith healing" to skew the results to make stents look like they help more than they actually do.
The importance of blinded studies like ORBITA that use sham procedures goes far beyond hearts and stents. They have yielded surprising and valuable findings on expensive procedures for knee arthritis and difficult-to-treat hypertension.
If doctors — and, more importantly, patients -- truly want to know what the best treatments are, we need more blinded studies with sham procedures and "hard outcomes" to eliminate the "faith healing" effect.
For now, if you have stable angina, it’s worth asking if you really need that stent. You might feel just as well if your doctor says you don't need it.
Top photo by Lenore Edman, second photo by Jason Bechtel, via Flickr creative commons