Support WBUR
Coming To A Clinic Near You: The $50 IUD With A Fascinating Backstory

Zoe Reiches got her first IUD this August — a new model with the lilting name Liletta.
Reiches, 25 and a human resources specialist in Boston, is now happily set for birth control for at least three years. “It’s convenient, I don’t have to worry about it, and I didn’t have to pay for it because of insurance,” she said. “I’m lucky in that sense.”
Millions more American women share her luck now that Obamacare has mandated birth control coverage with no co-pays for most insurers.
But the Liletta, which is just starting to roll out at clinics and hospitals here in Boston and around the country, is not only a device for the lucky — quite the opposite.
Its whole reason for being is to serve poor and uninsured women, to make IUDs — which can cost $1,000 or more — affordable to all, and available on demand at publicly funded health centers.
“This has never been done before,” said Jessica Grossman, the new CEO of Medicines360, the nonprofit pharmaceutical company behind the Liletta. “Our whole mission is to offer this low-cost product.”
Very low cost, compared to the usual thousand-plus dollars. At least until the end of the year, a special program guarantees that insured women who get a Liletta will pay no more than $75 out of pocket for it, Grossman said. A permanent patient assistance program will also provide Lilettas for free to women who qualify.
'Hey, I want an IUD and I want it now. I want it to be available to me today. I don’t want to come back.'
And, behind the scenes but even more important, public health clinics can order the Liletta for a mere $50 each.
In Massachusetts, all six Planned Parenthood clinics have begun to stock the Liletta, and it’s starting to enter “formularies” — the approved prescription lists — from major hospitals to cash-strapped community health clinics. Medicines360 reports shipping Liletta to 49 states, with more than half of the devices going to clinics that serve low-income patients.
The idea is to make the devices affordable enough that clinics can stock plenty, Grossman said, so that a woman can come in and say, “'Hey, I want an IUD and I want it now. I want it to be available to me today. I don’t want to come back.' ”
The Anonymous Donor
The Liletta is the latest chapter in the story of the great resurgence of IUDs in the United States, featuring billionaire investor Warren Buffett in a key cameo.

After the 1970s debacle of the Dalkon shield, which caused infections and even a few deaths, IUDs fell almost completely out of use among American women. Then, in 2001, a new, hormone-emitting device came on the market — the Mirena.
IUDs steadily gained popularity as a relatively safe, set-and-forget, long-acting but reversible option for many women. (As a no-complaints Mirena user for a decade, I’m one of them.)
More than 10 percent of American women who use birth control now choose IUDs, the most recent data show — the Mirena or the Skyla, which emit tiny amounts of hormones, or a simpler copper IUD, the Paragard.
The latest evidence of the IUD’s full rehabilitation: New York City’s Health Department this week launched its “Maybe the IUD” campaign to encourage New York women to consider an IUD.
The campaign talks about “reproductive justice,” reflecting in part a troubling trend: Unintended pregnancy is increasingly a poor woman’s problem. Look at the trend in the Guttmacher chart below:
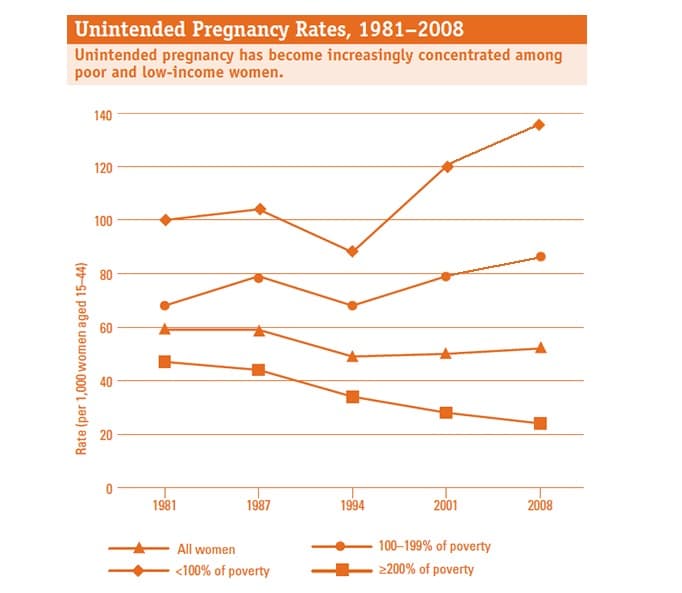
The numbers shout that poor women need more effective birth control. IUDs are over 99 percent effective and they last years. But they’re expensive.
"[So] people basically got together to say, ‘We need this option to be available to all women, not just those with resources or who have insurance,' ” said Guttmacher Institute senior research scientist Megan Kavanaugh. “That’s one of the main drivers for getting the Liletta out there — to increase access for all women.”
Yes, under Obamacare, IUDs should be free to women with insurance, but that leaves many women out, says Dr. Alisa Goldberg, director of family planning at Boston's Brigham and Women’s Hospital and director of clinical research and training at the Planned Parenthood League of Massachusetts.
They may lack insurance, she said, or be undocumented immigrants, or need to pay out of pocket for birth control for privacy reasons. The Liletta could help “women who are currently falling through a variety of cracks,” she said.
Thanks to epic reporting by Karen Weise at Bloomberg Businessweek, we now know that those family planners who got together to create a low-cost IUD had the financial backing of the billionaire Buffett’s family foundation. (Don't miss her recent piece: "Warren Buffett's Family Secretly Funded A Birth Control Revolution.")
Over $70 million in seed funding for the Liletta came from an anonymous donor, Weise writes; she followed a trail of "tax filings, medical journal disclosures, and an archived interview with a foundation official" to Buffett's family foundation, the Susan Thompson Buffett Foundation, named for Buffett's late first wife.

In 2009, Medicines360 came into being “with the sole purpose of developing a low-cost, hormonal IUD,” said Grossman, its new CEO. “That is our mission.”
Medicines360 licensed a European IUD very similar to the Mirena, Grossman said, and, with that money from a “single philanthropic donor” (she absolutely refused to name the donor but that’s OK because we know who it is), took it through the biggest American clinical trial yet for a hormonal IUD.
When the FDA approved the Liletta this February, results from that trial backed its use by a broad swath of women, including those who’d never had children, who were as young as 16, who were thin all the way up to very obese with a Body Mass Index of 50.
Medicines360 does not actually make or sell the Liletta; it has a commercial partner, Allergan, that does all that.
Allergan sets the commercial prices when a woman gets a Liletta through private insurance (Reiches says her plan was billed $1,400). But the deal is that all public health or “safety net” clinics get the Liletta wholesale for just $50.
“If clinics can’t afford to stock it, then they can’t offer it to their patients,” Grossman said. “So that’s where we come in, that’s our goal.”
Dr. Goldberg, who is on Medicine360‘s scientific advisory board, attests to the importance of that low $50 price. Clinics often can’t afford to stock many IUDs when they cost hundreds of dollars wholesale, she said. If a patient comes in and is told there’s no device immediately available, she may well not come back — or come back too late, already pregnant.
“I’ve seen that happen,” she said. “The patient came in for an IUD, couldn’t get it, got rescheduled for a later appointment — and it’s just a little too late.”
Rachel Preiss, a nurse practitioner and clinical manager at the Dimock Center, a community health center in Boston, says that when IUDs run out, “We’re all aghast.”
“All the studies show that if you can do it right now, women are more likely to be happy with it, they're more likely to continue with it,” she said.
The Liletta is not yet offered at the Dimock Center, but Preiss has signed up for Liletta training in November, she said, and is already calculating that its low price could quintuple the IUD stocks on the shelves.
IUD Nation?
So how far can the reborn IUD go? And will it make a difference?
Just over half of American pregnancies are unintended. A striking recent drop in teen pregnancies in Colorado, where that anonymous donor funded a free-IUD program, seems to suggest that the Liletta might help cut that rate. Teen abortions dropped by more than a third over a three-year period in the counties served by the program, and teen pregnancies by 40 percent statewide, according to the governor.
Studies have yet to be done at the national level, said Kavanaugh of the Guttmacher Institute, but it follows: If you move people to more effective contraception, you’re going to have lower rates of unintended pregnancies.
As for IUD rates, in other developed countries, the percentage of women who choose them tends to hover in the teens or 20s, Kavanaugh said. Norway is at 23 percent, France at 19. (Then there’s North Korea at 62 percent and China at 40 percent — different category.)
The Choice Project, a landmark St. Louis study also reportedly funded by You Know Who, found that when all cost barriers were removed, most women opted for the most effective, long-acting methods: 56 percent for IUDs and 11 percent for implants.
But that study had some special conditions, among them that the counselors used a special script that especially highlighted advantages of IUDs and implants, Kavanaugh said.
So it’s not clear what the American IUD rate will be — or what it should be.
It’s tricky territory, the intersection between fertility and class. There’s been some tension in the family planning field about how to talk about promoting long-acting methods to different groups of women, Kavanaugh said, with high sensitivity to possible “undertones of coercion.”
Preise reports in Bloomberg Businessweek:
This March, a state legislator in Arkansas proposed a bill that would pay unwed, low-income mothers on Medicaid $2,500 to get an IUD. That echoes a not-so-distant controversy over the Norplant hormonal implant. After it hit the market in 1991, legislators in more than a dozen states introduced bills that would have pushed women into getting the implant as a condition of welfare, in lieu of jail time, or in exchange for cash."
Issues of class and coercion aside, any family planning specialist will tell you that choosing a method is a highly individual issue, with no one-size-fits-all best method.
Preiss, of the Dimock Center, says that when she’s counseling women on contraception — one of her favorite parts of her job — and she brings up IUDs, “I don’t get a ton of takers.”
"I don't get a ton of takers [for IUDs]."
Nurse practitioner Rachel Preiss
“I’m finding right now we have a lot of people who prefer Depo-Provera, we have a lot more people using [the implant] Nexplanon right now,” she said. “We do have some IUD users and I don’t really know what it is that would help increase those rates, because the studies show that when people do choose an IUD, they use it for longer and they're more happy with it.”
Liletta's sales may also be slowed by its initial time limit of just three years, though the limit is expected to be extended to five years or longer after further study.
When Reiches was considering her Liletta, she heard a lot of IUD “horror stories,” she said, of pain and problems, even from family planning enthusiasts.
‘I felt like I was taking a risk,” she said. But in the weeks she’s had the Liletta, “I‘ve had a really positive experience so far.”
She would “hesitate to recommend anything to anyone, because it really is a personal choice,” but of one thing she is sure: “Education and access need to be available for everybody.”
Readers, IUD thoughts or experiences?
