Support WBUR
Chest Pain Is Top Item On Nation's $80 Billion ER Care Bill, Study Finds
If you're feeling chest pain that you think might be a heart attack, there's only one thing to do, medical experts say: Seek emergency care. Do not pass go, do not collect $200. Or rather, do not think about the roughly $1,000 your care will cost the hospital. Your life may be at stake.
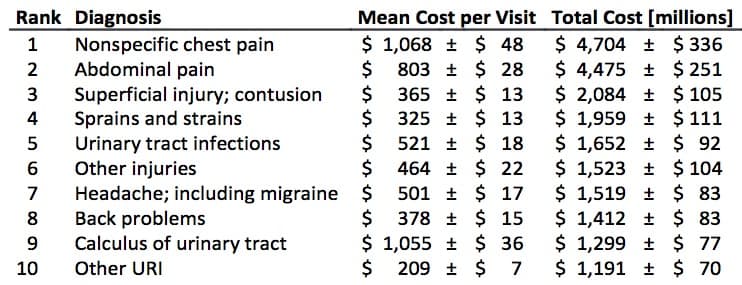
But at a calmer moment less fraught with risk, you might want to contemplate the bigger picture of chest pain and emergency care, as sketched out by Dr. Jonathan Slutzman of UMass Medical School and colleagues at a recent national conference on emergency medicine. To wit: Your costs are part of a national Emergency Department care bill that totals nearly $80 billion, including nearly $5 billion for chest pain alone.
Every year, Americans log a total of about 130 million visits to emergency rooms, Dr. Slutzman said. Among those visits, according to his team's analysis of millions of records, patients who come in for chest pain are the single biggest line item on the bill.
"Chest pain is one of the two most common reasons somebody comes into the Emergency Department," he said. "It's somewhere on the order of 5 percent of all visits," which may not seem like very much until you realize it's 5 percent of 130 million, and each chest-pain visit costs about $1,000.
The grand total: $4.7 billion. It's so high because chest pain is both a high-volume diagnosis and the treatment is high-intensity, Slutzman said, usually including blood tests, X-rays, sometimes CT scans and sometimes stress tests. They add up.
So now that we see that prodigious price tag, what is to be done?
Emergency medical specialists are working on that problem, he said, in part by figuring out what the "best practices" are for evaluating chest pain. "This is on people's radar screens," he said, "to try and 'rightsize' our care," meaning that "we can safely treat many patients while doing less."
To which I naturally responded: "Yikes. I don't really want the system to be trying to save money when I might be having a heart attack."
Slutzman calmed me down. His No. 1 takeaway from the findings, he said, is that more patients should probably be evaluated as to whether they're having a heart attack without having to stay overnight in a hospital. Chest pain patients tend to be almost reflexively kept in the hospital for at least one night of testing, he said, "and a big subset of those people don't really need it. One big key is more rapid access to outpatient providers. If someone can see their doctor in one to two days and maybe get some additional testing then, they can be safely discharged."
That calmed me down a bit. I do believe in staying out of the hospital whenever possible.
He calmed me still further with a story:
Historically, back in the late '80s and early '90s, if you walked into an Emergency Department with chest pain, you got admitted to a cardiac Intensive Care Unit, pretty much no matter what, because there was so much concern that they could be missing heart attack. There was a lot of fear of that.
And then, over time, we learned more and more. We could read our electrocardiograms — our EKGs — a little better, we could learn a little bit more about what the squiggles meant, and which ones were dangerous and which ones weren't.
And then we got more blood tests that were a little bit more sensitive and a little bit more specific, and a little bit better at figuring out who was having a heart attack and who wasn’t.
And then we thought, OK, we get the blood test when they first come in, and then we get another one eight hours later, and then another one eight hours after that, and then if they're all negative, we say they're not having a heart attack, over those 16 hours.
And then we learned, as tests improved, 'Wait a minute, actually, we don’t need that third one.' If the second one is negative, the third one is always negative, it doesn’t need to take 16 hours anymore. Maybe we can do it in eight hours.
And now the latest advance is that some subset of patients, we’re learning, we can probably say, 'You’re not having a heart attack' in three to four hours.
And it’s taken a long time, we’re talking about 20 to 30 years with a lot of dedicated researchers and a lot of innovations in diagnostic testing, and thousands and thousands and thousands and thousands of patients learning the better way to do this. I’m not going to say it's the best way, because we’re not there yet, but I think we’re getting better and I think that over time, we will continue to get better and figure out more effective ways to do these things.
And certainly, I prompted Slutzman, there are not just financial but medical downsides to being hospitalized?
Certainly, he said, particularly hospital-acquired infections. His attitude, he says, is that he doesn't care what a patient's insurance is; he doesn't ask; he provides the best care he can for every patient. "And lots of times I tell people, 'I strongly recommend that you not want to be admitted, because I think it's perfectly safe to take care of you as an outpatient, and it reduces your risk for all these untoward outcomes that happen to people in the hospital.' "
Readers, reactions?
And just one footnote: The analysis by Slutzman's team also found that ER treatment amounts to more than $1 billion a year for people who turn out to have nothing but the common cold.
Of course, some of those patients may have been having trouble breathing, and it's a good reason to go to an ER if you feel like you can't breathe, he said. But if you really just have a cold, you might want to just call your primary care doctor. Each of those Emergency Department visits cost only $200 or $300, he said, but they're so common that they add up to $1.2 billion.
