Support WBUR
The Price Of Health
Massachusetts, The Innovation Hub, Debates Aggressive Drug Price Controls

Deidre Waxman climbs onto a stone bench outside the Massachusetts State House, about a mile from the world-class hub of drug development in Kendall Square.
"We need change. We need affordable meds. And I need my insulin," Waxman shouts to about 100 health care consumer advocates who've gathered for a rally.
Waxman says the only way she can afford insulin is to buy it in Canada, where she saves $1,200 a month.
"Should we be needing to cross borders to buy life-saving medication?" Waxman asks. "No," the crowd calls back.
Waxman is with the Right Care Alliance, one of 16 health care organizations backing a broad bill organizers say will make drugs more affordable in Massachusetts.
The first step in the bill would require manufacturers to explain how they set a drug price the state considers "unreasonable or excessive." Pharmacy benefit managers, the middlemen such as Express Scripts and OptumRx, would also be called to testify about their role in deciding how much drugs.
"It's very complicated, it's a black box for most people," says the bill's Senate sponsor, Democrat Jason Lewis. "We need to hold drug manufacturers and pharmacy benefit managers to the same standards as we do other participants in the health care system."
Lewis is referring to annual reports that hospitals, physician groups and health insurers file with the state. These groups also testify at annual hearings on health care cost trends, which have not, to date, included the pharmaceutical industry.
"They're not asking us to play by the same rules; they're asking for more," says Robert Coughlin, president and CEO of MassBio, a industry trade group representing more than 1,200 companies and organizations.
The "more" is a part of the bill that calls for drugs with excessive prices to be referred to the state attorney general as a possible violation of consumer protection laws, cementing the AG's role in a drug price review process. That provision is seen by some in the biotech industry as a threat.
"It will certainly have a chilling effect on economic development here in Massachusetts," Coughlin says.
Baker's Bill
This back-and-forth between the pharmaceutical industry and advocates pushing to lower drug costs provides a glimpse of the contentious debate unfolding in public and behind closed doors on Beacon Hill. The opening chapter will close any day now because plans to tackle rising drug costs within MassHealth, the state's Medicaid program, are included in a new state budget that would take effect July 1.
Gov. Charlie Baker opened this chapter in January when he requested authority to negotiate deeper discounts with a few drug companies. Baker said he would focus on the most expensive drugs, those that cost $25,000 per patient, or those for which the state's total annual expense was more than $10 million after rebates.
That might include Harvoni, a drug that cures Hepatitis C, for which the pre-rebate cost to MassHealth in 2018 was $116.8 million, or Suboxone, an addiction treatment that cost $73.7 million. Another expensive drug, Keytruda, a cancer immunotherapy treatment, cost the state $29.7 million before rebates.
The Baker administration says it is not allowed to disclose the actual spending totals, after rebates, for these drugs.
In an email exchange, a spokeswoman for the U.S. pharmaceutical industry trade group PhRMA noted that MassHealth already receives "the best price for medicines under by federal law." And she says that PhRMA discounts or rebates reduce MassHealth's overall cost for medicines by 55%.
But even with existing rebates, Baker says pharmaceutical spending in Massachusetts has nearly doubled since 2012. He estimates that negotiations to lower the price of the most costly drugs would save the state $70 million a year.
Both the House and Senate added parts of Baker's MassHealth drug price negotiation plan to their budgets, but the House left out some of the key pressure points, including referral of the most egregious prices to the AG's office. A spokeswoman for Attorney General Maura Healey says she is reviewing these proposals and has no position on them at this time.
The Upper Payment Limit Provision
Now, as a committee tries to resolve these difference and others, it looks like the state budget will be late. Whatever happens in the budget will set the stage for an even more vigorous battle this fall. The trigger: something called an upper payment limit.
The upper payment limit is part of the bill backed by a coalition including Health Care for All, the Massachusetts Medical Society, the Greater Boston Interfaith Group and 1199SEIU, the largest union of health care workers in the state. It would allow the state's Health Policy Commission (HPC) to review the value and cost of the most expensive drugs and set caps on insurance or consumer payments for those found to be "excessive or unreasonable."

Generic drug prices that rise more than 15% a year would also be subject to review. And any cap would apply to all purchases of these drugs in Massachusetts.
It's the best way to "ensure accountability throughout the system so that drugs are more affordable for consumers," says Alyssa Vangeli, co-director of policy and government relations at Health Care for All.
Two other states, Maryland and Maine, have passed laws that include an upper payment limit for very expensive drugs, but the Massachusetts version is the most expansive and would take effect sooner than other states. It also has teeth with referral to the AG.
Trish Riley, executive director at the National Academy for State Health Policy, who helps state lawmakers draft drug affordability bills, says the upper payment limit is based on the idea of life-saving medicines as a public utility that must be accessible to everyone.
"The goal is to try to get a handle on what an appropriate price should be," Riley says. "Clearly consumers have made abundantly clear that the prices of drugs are beyond the pocketbooks of affordability."
Riley says Massachusetts could move more quickly than other states to create an upper payment limit because it already has the HPC, an agency that studies health care costs.
Coughlin counters that the HPC doesn't have the expertise right now to decide what a drug should cost.
Why, he asks, would you "establish the most far reaching, rigorous government involvement on the best place in the world for this industry? It makes no sense."
Outside the State House, Waxman, the patient advocate, offers an answer to Coughlin's question.
"Human need, not pharma greed, that’s what we want," Waxman says to a round of cheers.
A WBUR poll out this week found that 77% of Massachusetts residents list the push for maximum profits as a top contributor to drug prices.
Coughlin says that’s not what’s happening inside his member companies.
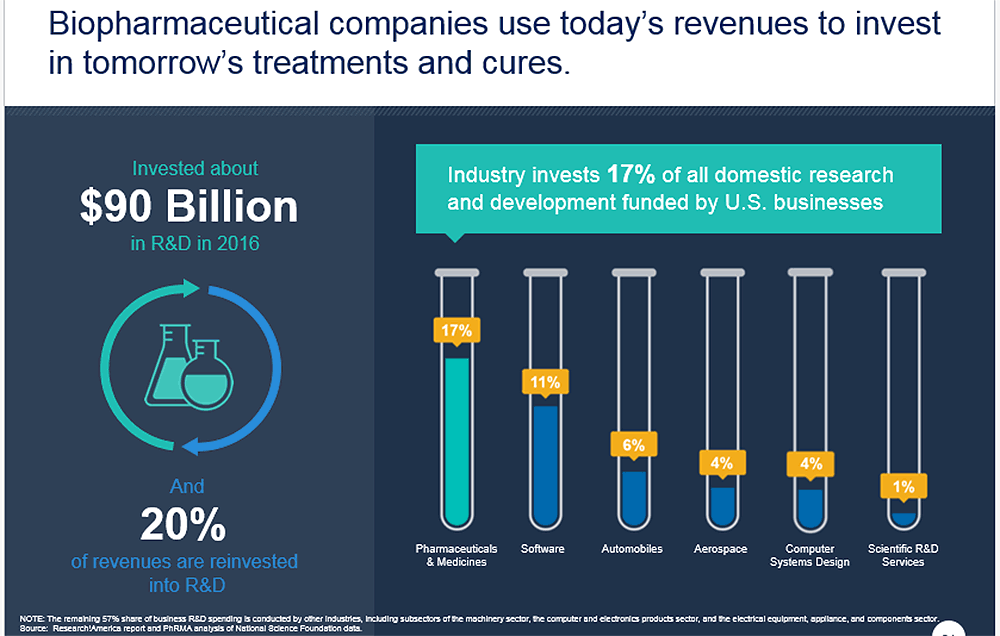
"What they’re doing is trying to create an environment in which they can raise money to actually do research," he says. "The drugs we’re paying for today invent the drugs of tomorrow."
Industry figures show pharmaceutical companies reinvest 17% of revenue into research and development, which PrRMA says is more than any other manufacturing sector. Consumer advocates see that figure as proof that biotech companies could lower drug prices and still have plenty of money to fund the search for new drugs.
But studies show that 17% would shrink if regulators cut PhRMA profits because "the expectation of future profit is what drives innovation," says Dr. Anupam Jena, a health economist at Harvard Medical School, who consults with biotech companies on the economic value of new drugs.
The question, Jena says, is whether society would be giving up a cure for cancer or HIV or some marginal improvement in treating high blood pressure in order to have more affordable drugs.
For Baker, the tension boils down to this: "At the end of the day, for drugs to be accessible to people, they need to be affordable."
Baker says his administration has invested in life science research and jobs. Now he says, it’s time to balance support for the industry with efforts to rein in the highest drug prices. Baker mentions his MassHealth negotiation plan and the steps he'd use to hold drugmakers accountable for high prices.
"I don’t think that’s unreasonable," Baker says. "It’s a fact-based process, it’s a public process, and it’s one that is only going to apply to a certain number of drugs in certain circumstances."
Riley says states have been and will continue to be important labs for testing ways to make drug prices more affordable. Requiring more information about how prices are set is the most common current approach. Four states have passed laws that would allow consumers to buy medicine in Canada, but they need federal waivers to move forward. And there may be other legal delays.
"Anything a state enacts is likely to face court challenge from the [pharmaceutical] industry," Riley says.
This article was originally published on June 28, 2019.
This segment aired on June 28, 2019.
