Support WBUR
Doctors Who Actually Tackle Your Unhealthy Lifestyle
"You should lose weight and exercise, but in the meantime, take these pills."
That's the sort of prescription Dr. Damian Folch, a general practitioner in the working-class Massachusetts town of Chelmsford, might have given a typical patient in the old days.
But Dr. Folch has changed, radically, under the influence of an emerging movement called Lifestyle Medicine, centered in part here at Harvard Medical School. And if health reform goes as expected at both the national and the state level, many more doctors may undergo similar transformations, in keeping with strong new incentives to keep patients well rather than just treating them when they're sick.
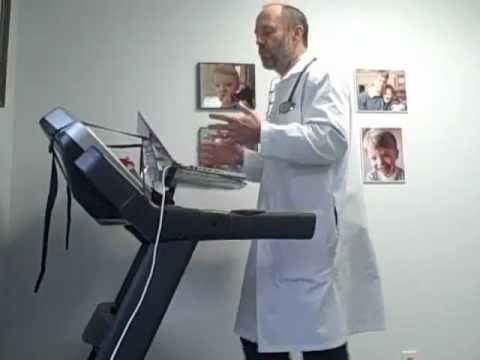
Dr. Folch doesn't just tell patients to eat better and get moving, he coaches them using proven motivational techniques. He records the amount they exercise as a vital sign, along with blood pressure and pulse. He writes out prescriptions for exercise on his pad. He shows them his office treadmill desk and shares his own fitness efforts, which include his first-ever half-marathon this fall at the age of 58.
[module align="right" width="half" type="pull-quote"]'Medicine’s past was dominated by fighting infectious disease; its future is dealing with chronic disease influenced by lifestyle.'[/module]
A national survey by the CDC just reported that more than ever, doctors are advising their patients to exercise: In 2010, 32% of adult patients reported being told to exercise, up from about 22% a decade earlier.
But it's not enough to just say, "You need to exercise." Or "Please eat less." Lifestyle Medicine teaches doctors how to actually get their patients to do it — as part of an evolving science of healthy behaviors.
The evidence is mounting that a doctor’s guidance can have dramatic effects. A Brigham and Women’s Hospital study of more than 30,000 patients with diabetes found that “lifestyle counseling” helped them improve their glucose scores, blood pressure and cholesterol far more rapidly than usual care, this month’s “Diabetes Care” journal reports.
Similarly, two recent New England Journal of Medicine papers found that “lifestyle coaching” significantly helped patients lose weight.
A no-brainer, but revolutionary
It seems like a no-brainer, acknowledges Dr. Edward Phillips, director of the Institute for Lifestyle Medicine at Harvard Medical School. Doctors and patients alike know they should eat right, exercise, stay trim, quit smoking. At the same time, what Lifestyle Medicine proposes is downright revolutionary:
“We’re seeking nothing short of transforming the practice of primary care,” he recently told a lunch-time meeting of interested Harvard medical students.
His argument: More than half of deaths involve poor lifestyle behaviors like unhealthy diet and inactivity. The World Health Organization predicts that by 2020, two-thirds of disease will stem from lifestyle choices.
Medicine’s past was dominated by fighting infectious disease, he says; its future is dealing with chronic disease influenced by lifestyle.
Yet the current model of medicine amounts to only “taking care of something once it’s broken” — and that, he argues, “is not sustainable anymore.” Medicine must be “redirected.” Doctors have to actively help keep people well instead of just treating them when sick.
How? Dr. Phillips distilled what the Lifestyle Medicine movement aims to do to change the practice of medicine:
- Teach students of health care much more about exercise, nutrition, stress and other lifestyle topics.
- Give doctors better tools for helping patients change, such as exercise prescriptions.
- Help doctors improve their own lifestyle behaviors so they can better motivate patients. (The institute offers an annual course called “Active doctors, active patients” that even includes gym time for doctors.)
- Emphasize training for doctors on how to coach their patients rather than just issue commands.
The advent of Lifestyle Medicine couldn't be more timely, he notes: "Accountable care organizations" that are financially responsible for keeping patients healthy are on the rise, particularly since new federal health reform rules that kicked in January 1. "Yet doctors and hospitals need training in how to promote healthy behaviors."
Barriers and challenges
Lifestyle Medicine is a whole newborn discipline already, with an American College of Lifestyle Medicine and its own journal and a landmark paper in the Journal of American Medical Association in 2010 defining its “core competencies.”
[module align="left" width="half" type="pull-quote"]'Time and payment, that combination is the big elephant in the room.'[/module]
But in some ways, it is still struggling uphill.
First, American medicine is notoriously conservative and slow to change. Enough said.
Second, at a recent Lifestyle Medicine conference at Harvard, one speaker referred to an “elephant in the room”: The threat of lawsuits. Doctors may fear that a patient might start exercising on their advice and then have a heart attack or other complication, and sue. (Dr. Phillips responds that he, instead, ponders the possibility of a physician who ignores nearly 10,000 articles on the benefits of exercise being sued for not prescribing exercise.)
In fact, even Lifestyle Medicine enthusiasts see two far bigger obstacles than fear of litigation: Money and time.
Michael Barry, executive director of the American College of Preventive Medicine, applauds Lifestyle Medicine as a growing movement, but says that one of its central challenges is what it lacks: “A core economic driver like other treatments. The pharmaceutical industry and the device industry, they’re economic drivers. We don’t see that with Lifestyle Medicine.”
Sigh. And then there is that ugly word: reimbursement. Health insurers don’t tend to pay for many of the processes of Lifestyle Medicine. How do you code for “discussed eating fruit instead of chips while watching television”?
Then there’s the eternal office time crunch. “A lot of physicians will push back and say, “We’re being squeezed so much within the current health care system,” Mr. Barry said. “We’ve got 10 minutes with a patient, and the patient comes in with ailments.” Adding a Lifestyle Medicine component, they may argue, “puts more on our plate.”
Actually, he said, “it’s really not that overwhelming in terms of building it into your practice. A lot of it is mindset, and how you think: You think to prevent.”
But time is a tough one, even Dr. Folch of Chelmsford allows. The elephant in the room is not fear of lawsuits, he said. “Time and payment, that combination is the big elephant in the room. And that should get better with health reform.”
The coming waves
Indeed, health care reform and Lifestyle Medicine fit together neatly. A central tenet of reform, particularly here in Massachusetts, is that instead of “fee for service,” in which doctors are paid for each bit of care they provide, the system should focus on overarching care that is paid for in a big “bundle” — with bonuses for good results.
[module align="left" width="half" type="pull-quote"]'You're going to get paid based on your patients' blood sugar measurements or body mass index.'[/module]
As Dr. Phillips warned the Harvard students, the federal health overhaul includes a provision under which “you guys may, in the near future, get paid based on the health behaviors and outcomes of your patients. When that day comes, and the metric shifts 180 degrees, I would just say to be ready. You’re going to get paid based on your patients’ A1Cs [a blood sugar measurement] or BMIs.”
Another tenet of reform is that doctors must become less like lone cowboys and more like good team players. Lifestyle Medicine fits into that perfectly. Take the study on 30,000 diabetics. Dr. Alexander Turchin of Brigham and Women’s Hospital said that it’s clear that there are not always enough “physician resources” in the system to perform the counseling that the study found was so helpful.
“So we do need to be more creative to implement findings like this,” he said. “We may need to engage more nurse practitioners or physicians assistants, more dietitians. Or maybe do group counseling, which is more cost-effective.”
But something must be done. “Lifestyle is the cause of many of these diseases,” Dr. Turchin said. “So lifestyle really does need to play a role in dealing with it as well.
What a practice looks like
Back to Dr. Folch’s office in Chelmsford. He’s so busy — a solo practitioner with a roster of 3500 patients — that he has recently expanded and added two new staffers to his team, a physician's asssitant and a nurse practitioner, who can help with Lifestyle Medicine-based care.
The office has expanded physically as well, which let him put in a shower for after lunchtime workouts. “You lead by example,” he says. Lifestyle Medicine conferences influenced him to ramp up his exercise to the point that he’s in the best shape of his life. He went from size 34 to size 30 pants, and he gets comments from patients like “Wow, you look great! What have you been doing?”
During a recent morning of office hours, he saw a broad gamut of patients, from a generally healthy fortyish blonde seeking more holistic care to a developmentally disabled man with diabetes to an elderly man with congestive heart failure.
He shared exercise guidelines and recommendations on books about healthy eating with the fortyish woman, explaining how to lift weights to the point of muscle failure. She complained of having the hips of a 70-year-old, and he suggested Vitamin D to help her bones absorb calcium. (His practice has recently added a website with a compendium of Lifestyle Medicine resources.)
A young man who works in a warehouse had recently gained five pounds despite more than a week of diarrhea, and Dr. Folch told him straight that the extra weight was driving up his high blood pressure. “Do you exercise?”
“I play ball sometimes.”
Dr. Folch turned to the man’s wife and asked if they might go for half-hour walks together. “If you lose weight, you could not need medication,” he said.
But perhaps the star of the morning was the 83-year-old woman who had quit smoking three months ago after 50 years of more than a pack a day. Dr. Folch referred her for lung rehabilitation, and dealt with other medical issues, but perhaps this was his most potent medicine of all:
“Wow,” he told her, eyes alight with pride. “I’m so impressed!”
Further reading
This program aired on February 17, 2012. The audio for this program is not available.
