Support WBUR
U.S. Health Care Is Less Private, More 'Socialist' Than You Might Think
By Richard Knox
Readers, a pop quiz:
The proportion of U.S. health care paid by tax funds is (a) less than 30 percent, (b) about half or (c) more than 60 percent.
If you picked "more than 60 percent," you’re right -- but you’re also pretty unusual.
“Many perceive that the U.S. health care financing system is predominantly private, in contrast to the universal tax-funded health care systems in nations such as Canada, France or the United Kingdom,” David Himmelstein and Steffie Woolhandler write in a new analysis of U.S. health spending in the American Journal of Public Health.
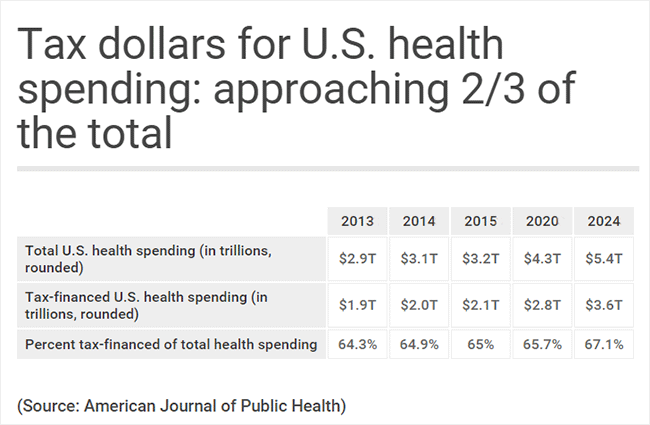
They find that 64.3 percent of U.S. health expenditures are government-financed. And they project the tax-supported proportion will rise to 67.1 percent over the coming decade as the baby boom generation ages and retires -- nearly as high as Canada’s 70 percent.
“We are actually paying for a national health program, we’re just not getting it,” Woolhandler says.
Now, Himmelstein and Woolhandler have an agenda. For decades, they’ve been perhaps the leading researchers promoting the kind of single-payer health system that Socialist and Democratic presidential candidate Bernie Sanders has put on the debate agenda. One recent poll suggests more than half of Americans (and 30 percent of Republicans) support the idea.
But even if you disagree with the Himmelstein-Woolhandler ideology, their research is generally regarded as sound, and their method is straightforward.
They added up what federal and state governments spend on health through Medicare, Medicaid, the Veterans Health Administration, government employees’ health care premiums, tax subsidies and other programs. They argue that accounting by government agencies (the Center for Medicare and Medicaid) undercounts the real tax burden because it leaves out major pieces of the pie -- such as government employees’ care ($156 billion a year) and tax subsidies for private, employer-sponsored coverage (nearly $300 billion).
And whatever you think about Medicare-for-all, it’s a good idea to see the present U.S. health care system for what it is — an increasingly government-funded financing scheme.
That’s because, however this political season unfolds, you’re going to hear a lot more claims about what’s wrong with the U.S. health care system and how to fix it. Beyond the debate between Sanders and Hillary Clinton over Medicare-for-all versus the Affordable Care Act, or Obamacare, the Republicans are expected to put forward their ideas on replacing Obamacare.
The more you know about the way the current system works, the better able you’ll be to sort through the blizzard of reform ideas.
So here are some facts to take on board from the Woolhandler-Himmelstein paper and other sources:
- The predominance of tax support in our current system is not just because of Obamacare. It’s been happening for decades. In 1965, before the enactment of Medicare and Medicaid, about one in every three health care dollars was government-funded. By 1980, a little more than half was. Even before Obamacare was passed in 2010, tax dollars accounted for at least 60 percent of the nation’s health care bill. No matter what happens, this trend will not be easy to reverse.
- The other standout feature of the U.S. health care system is its highest-in-the-world cost. No other nation comes close to the $9,267 cost-per-person of U.S. health care. But even more striking, according to the new analysis, the total health care bill of every other country except Switzerland is lower than what America spends on just the tax-funded portion of its bill -- nearly $6,000 per person.
- Here’s another cost yardstick: how much health care consumes of national wealth, as measured by gross domestic product, the total value of all goods and services. In the U.S., it’s more than 17 percent, again the world’s highest. But consider this: Just the tax-funded portion of U.S. health care — 11.2 percent of GDP, according to the new paper -- is more than any other nation, including all those that are totally tax-supported.
- Momentum is not on the side of health care cost control. The U.S. health care bill just passed $3 trillion a year -- 20 percent higher than just seven years ago -- according to new government figures in the current issue of Health Affairs. That total bill is bound to increase in coming years because of the graying of America and other factors, such as expensive medical innovations. (Just one recent innovation -- new drugs to cure hepatitis C -- had substantial impact on total drug spending, government analysts say.) Even modest rates of medical inflation loom large when applied to such staggeringly high spending.
These facts and trends should be kept in mind while weighing political arguments over health care.
For instance, take the recent back-and-forth between Sanders and Clinton. Sanders can take heart from the Himmelstein-Woolhandler analysis, because it shows the nation is already most of the way toward a totally tax-funded health system.
“We’re not that far away from collecting the taxes we would need to pay for a single-payer system like Canada’s,” Woolhandler says. “We already pay so much in taxes for health care that it’s not that big a stretch.”
In the most recent Democratic candidates’ debate on Jan. 17, Sanders said his plan would offset the needed tax increase to fund Medicare-for-all by abolishing private health insurance premiums. “My proposal -- provide health care to all people, get private insurance out of health insurance -- (would) lower the cost of health care for middle-class families by 5,000 bucks,” Sanders said.
Clinton countered that Sanders’ plan is politically unrealistic. She pointed out that even when the Democrats controlled Congress, they couldn’t pass a more modest proposal -- allowing Americans to “buy into” Medicare. “There are things we can do to improve [Obamacare], but to tear it up and start over again, pushing our country back into that kind of a contentious debate, I think is the wrong direction,” Clinton said.

But one important aspect of that debate got little attention -- the failure of Vermont, Sanders’ home state, to implement Medicare-for-all. Sanders slid by a question on that. “You might want to ask the governor of the state of Vermont why he could not do it,” he said.
By one recent analysis, the cost of the project is what sank it.
The administration of Vermont Gov. Peter Shumlin figured it would cost the state $2.5 billion to implement a single-payer health system. “The state only raises $2.7 billion in taxes a year,” journalist Sarah Kliff pointed out this week in Vox. “The single-payer plan would mean doubling tax collections. ... That’s a big lift even if it would replace existing health premiums.”
Kliff says totally government-financed health care needn’t cost Vermont $2.5 billion a year. But she says making it affordable would require a massive rollback in payments for doctors, hospitals, pharmaceuticals and diagnostic tests such as MRIs, to levels comparable with those across Vermont’s border with Canada. That’s an even heavier political lift.
Woolhandler takes issue with that analysis. “The main lesson from Vermont is you do need a national program, or at least national support for a state program,” she says. After all, that’s how Massachusetts was able to implement its more modest Obamacare precursor program in 2006.
Woolhandler says Vermont could have squeezed more administrative costs out of health care than it was planning to do. And she said it’s “a piece of mythology” that doctors and other health care providers would have to be impoverished to make a single-payer plan affordable.
So the feasibility of Medicare-for-all isn’t yet clear. But at least the debate is venturing into territory never before covered in a national political debate.