Support WBUR
Eva Gets A Mammogram: A Primer On Finding Quality In Mammography

Eva Kennedy walks out of a dressing room clutching the strings of her pink and white johnny. Her face is calm, but her eyes flick nervously from person to person.
"I'm ready, I guess," says the 43-year-old mom from Harvard, Massachusetts. "It's kind of strange to have someone manhandling your breasts, smushing, just weird."
For the next 30 minutes this elementary school teacher will follow, not give, instructions. It's time for Kennedy's annual mammogram.
Millions of women across the country stand with Kennedy every year, in a johnny, in front of a machine that will compress their breasts and X-ray the pancaked tissue.
Most women assume a mammogram’s a mammogram -- you just get through it. But in fact the quality -- as with most things in medicine -- does vary.
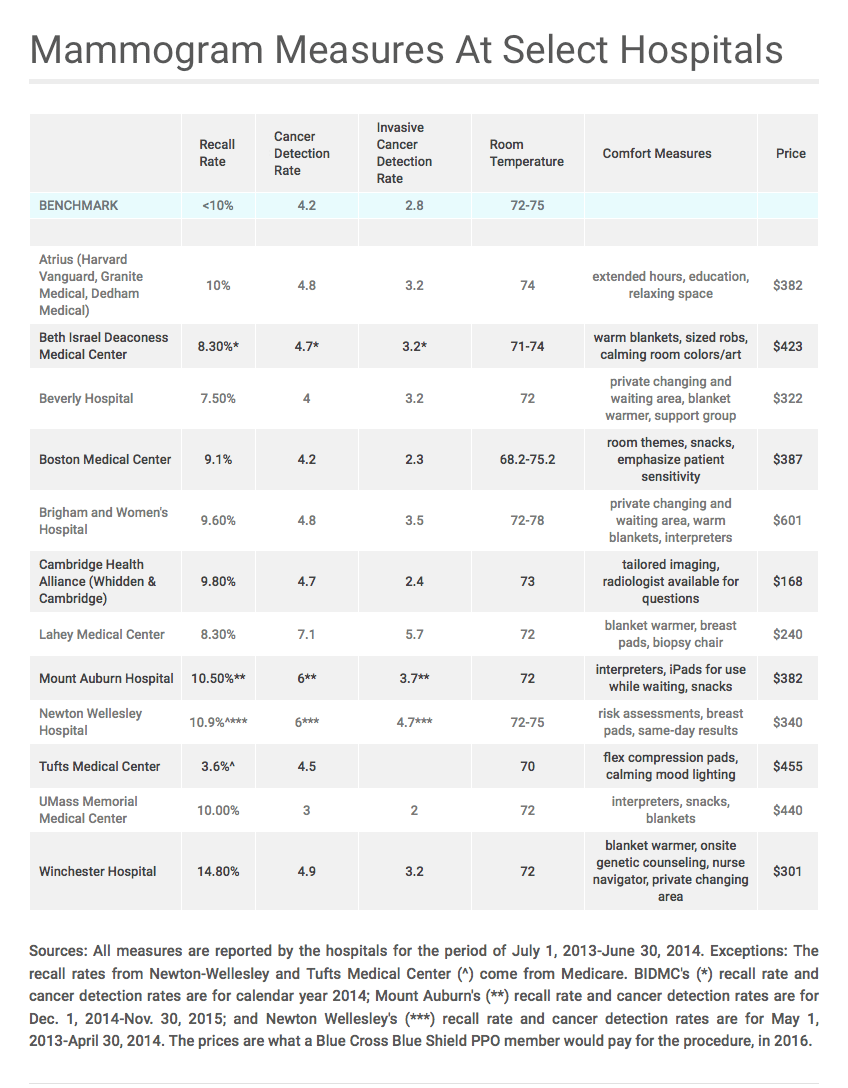
Here, for the first time, you can compare the quality of a mammogram at some of the larger hospitals and medical practices in Greater Boston and Worcester.
If you’ve had a mammogram or plan to get one, you may not have given much thought to where you should go. We hope to help you understand your choices by beginning a conversation about how to measure quality in mammography. Our data collection is not the definitive answer. But many women are surprised by the fact that where you get a mammogram can make a difference in your health.
"I was never told anything about that. I don’t think it’s out there," says Kennedy, who's come to the Beth Israel Deaconess Medical Center clinic in Lexington for a routine screening mammogram.
We collected information on five quality measures from a dozen hospitals that were willing to discuss how they perform when it comes to mammography. In addition to the table above, we have a detailed explanation of the project and the quality measures, as well as what each hospital is paid by one insurer for the test — just click here for that.
But let's stay with Kennedy, in the exam room, where you'll see why comparing quality matters.
This mother of two steps up to the machine with Ethel Waite, a radiologic technologist, at her side.
"All right, now lean back just a little bit," Waite says, stretching out the "e" in lean. "I want you to bring your right arm up by your head. And you’re going to drop this shoulder down," Waite says, placing her own hand on Kennedy's left shoulder.
That light touch is a subtle way of telling Kennedy to relax.
"It’s very difficult to use the word 'relax' in this room; as soon as you ask someone to relax they tense up," Waite says after the exam. "It’s a high-anxiety exam, so they’re very tense."
Waite needs Kennedy to relax so that Waite can get as much tissue as possible on the flat plate that will compress Kennedy’s breast. If some tissue is tensed up, around muscle, a radiologist might miss an area that could contain cancer.
"You really just need to be Gumby in here," Waite says. "You can get ... a lot more tissue if a patient is relaxed. When you’re very tight and taut it’s very difficult."
Waite takes two images of each breast -- a total of four X-rays that a radiologist will compare to Kennedy’s last mammogram.
"What they’re looking for is a change in your breast. If they find a change, you’re going to need a different exam," Waite tells Kennedy. "In that case I’d give you a call at that phone number that you wrote down. OK, don’t move," Waite says in a calm, reassuring voice. "No change, no call."
Waite dashes between her patient and a control panel about 10 feet from the machine, trying to limit the time Kennedy is clamped between two plates. A radiologist will review Kennedy's images later the same day. If the radiologist sees something of concern, Kennedy will be asked to return for a second set of tests.
Between 5 and 12 percent of patients (page 29 here) should expect to be called back for a second mammogram, according to the American College of Radiology. This is known as the recall rate. There's a fourfold variation in the recall rate among the hospitals we surveyed for this story.
(You can see the recall rate for many hospitals around the country on the federal government's site, Hospital Compare. It's the only mammogram quality measure that's been public, until now.)
No woman wants to hear that her mammogram shows something that could be cancer. But Kennedy got that call as she left school one afternoon, before a holiday weekend.
"I was, uh, trying to talk myself down since they called on Friday," Kennedy says three days later, when she's back in the breast imaging office. Kennedy, whose mom is a breast cancer survivor, spent the weekend going over all the possibilities, again and again, in her mind.
"Well it could be, not even cancer, but like a cyst," Kennedy says, rehearsing the optimistic outcome. Or maybe "I’d have to have biopsy." She tries not to think of what might happen next.
There are lots of reasons a mammogram may look different from one year to the next and trigger that call. The X-ray may be slightly blurred if the patient moves just a little. A mammogram will look different if the woman has lost or gained weight, which can change the density of breast tissue.
"The breast is actually a pretty complicated organ," says Kennedy’s radiologist, Dr. Peter Gross, a few days after reviewing her test. In Kennedy’s case, he says, there may have been a slight change in the position of her breast on that metal plate that created a worrisome image.
"It’s very difficult to position the breast in the same way for comparison and sometimes a little bit of tissue that was next to a different area simulates a mass," Gross says.
To be sure there was no mass, Kennedy had an ultrasound and two more X-rays of her right breast. She says the second mammogram was much more uncomfortable than the first.
"This time [the technician] had to add pounds of pressure, yeah," Kennedy says with a grimace. There was an increased "amount of squishing," she says.
It may have felt like more squishing, but Gross says the second test is actually the same amount of pressure. The difference is that it’s concentrated in a smaller area, which can feel more painful.
"Why can’t they just do an ultrasound?" Kennedy asks. It wasn't painful. And Kennedy didn't like the fact that she had six doses of radiation -- four images in her first mammogram and two with her second. "That’s, like, a lot of X-rays," Kennedy says.
One recent study that compared ultrasound and mammography says the cancer detection rates are comparable. Ultrasound did a better job of finding invasive cancer, the study found, but missed more small calcifications and had a higher rate of false positive tests as a whole. Many doctors say they'll continue to use ultrasound as a back-up for mammography.
Kennedy waits for the results of her second test and walks out of the exam room grinning.
"Everything was fine," she says with a deep sigh. "There’s no problems and I don’t have to come back for a year."
Kennedy is relieved. For most women, the second set of tests is negative. But the cancer detection rate does vary; there's a more than twofold difference among hospitals we compare.
The American College of Radiology says doctors should find cancer in at least 2.5 patients per 1,000 (again, page 29) who have a screening mammogram. The benchmark, or optimal, rate is higher -- at 4.3 cancers for every 1,000 patients, according to the Breast Cancer Surveillance Consortium, which is funded by the National Cancer Institute. All of the Massachusetts hospitals that submitted data for this story are within the acceptable range of 2.5 or higher.
A clinic or hospital's cancer detection rate is important, but some types of cancer are believed to be more dangerous than others. So we asked hospitals to break down their overall detection measure and show the rate at which they find cancer that is spreading in the breast, which is known as invasive cancer.
"The invasive cancer detection rate is a bit of a proxy for, are we finding the cancers that matter?" says Dr. Janie Lee, director of breast imaging at the Seattle Cancer Care Alliance. If the cancer is invasive, meaning it has spread beyond the ducts, “then it also has the potential to spread elsewhere in the body,” Lee says.
There is no optimal invasive cancer detection rate. The average rate for all hospitals that report to the American College of Radiology is 2.8 among 1,000 women who had a screening mammogram. The hospitals that sent in numbers for this story hover around that U.S. average.
'A Very Beginning State' For Comparing Mammograms
"In the Boston area, the quality of mammography overall is very good," says Dr. Tejas Mehta, co-director at Beth Israel Deaconess Medical Center’s breast care center. Mehta says clinics collect and report more information about mammography than any other test.
Many started when the Mammography Quality Standards Act became law in 1992. It set guidelines for the test, machinery and the training of personnel.
The act improved quality in mammography, "but there were still big differences from one place to another," says Dr. Richard Wolk, a retired radiologist who conducted audits of mammography labs for the American College of Radiology.
He says he saw widespread gaps in the quality of images, record keeping, follow-up efforts when patients needed a second mammogram and the rates at which doctors would require a biopsy.
At least one group collects and discusses mammography quality data with the goal of reducing disparities in the screening and treatment of breast cancer. Radiologists say mammography is well ahead of other medical tests in defining and reviewing quality.
But with mammography, like most tests and procedures, patients have had no objective way to figure out where to seek the best care for the best price.
"From the point of view of a consumer or patient trying to figure out what to do, I’d say we’re in a very beginning state," says Dr. Don Goldmann, the chief medical and scientific officer at the Institute for Healthcare Improvement in Cambridge. "I hesitate to use the word primitive, but we’re not where we need to be by any stretch of the imagination."
The six means of comparison we publish here are just a start. Radiologists have a number of cautions about how to review the numbers.
"No one performance metric can be evaluated in isolation," says Elizabeth Burnside, breast radiologist and vice chair of health services and outcomes at the University of Wisconsin School of Medicine and Public Health. "The most important benchmark when evaluating a breast cancer screening program is cancer detection rate with the added nuance that screen detected cancers should be small and early stage."
We do not have information about how often radiologists in Massachusetts detect cancer at an early stage. Or about the rate of biopsies done that didn't show cancer and thus may have been unnecessary.
Some physicians urge patients to ask who is reading the mammogram and to ask for a radiologist who specializes in breast imaging. Others stress that volume matters; physicians who read more than the required number of mammograms (960 every two years) may be more accurate than physicians who just meet the minimum standard.
We do not distinguish here between 2D and 3D mammography because quality benchmarks are the same for both tests. Some radiologists at hospitals that have switched to 3D tests say they are convinced that the newer, more expensive test is better. They say it's time for all insurers to cover 3D mammography. Insurers that don’t cover 3D point to organizations, like the National Cancer Institute, that say it’s unclear at this time if 3D mammograms are better than the 2D version.
This story does not dive into controversies about the kind of mammogram you should get or how often. Or whether mammography is even a valuable test at all.
But if you are shopping for a mammogram, take a minute to compare these measures. We hear a lot about comparing cost and quality to find the best value in health care, but very few doctors and hospitals give patients that information. When it comes to this one test, a small group of hospitals is helping patients determine what value in health care means.
Correction: An earlier version of this story said the Breast Cancer Surveillance Consortium is a division of the National Cancer Institute; it is funded by the institute. We regret the error.
This article was originally published on March 07, 2016.
