Support WBUR
6 Ways For You To Start Comparing The Quality And Cost Of Mammograms
If you’re a woman approaching or well into middle age, getting a mammogram every year or two may become routine. And you may assume that the experience and the results will more or less be the same at every hospital.
But quality and costs do vary. Here, for the first time, you have a glimpse of the range.
This is the beginning of a conversation about how to compare quality in mammography, based on guidance from dozens of experts in the field. We narrowed down a list of quality measures established by several national groups, then wrote to 14 hospitals — some of the largest providers in the state — and asked for their data. Twelve agreed to release the data.
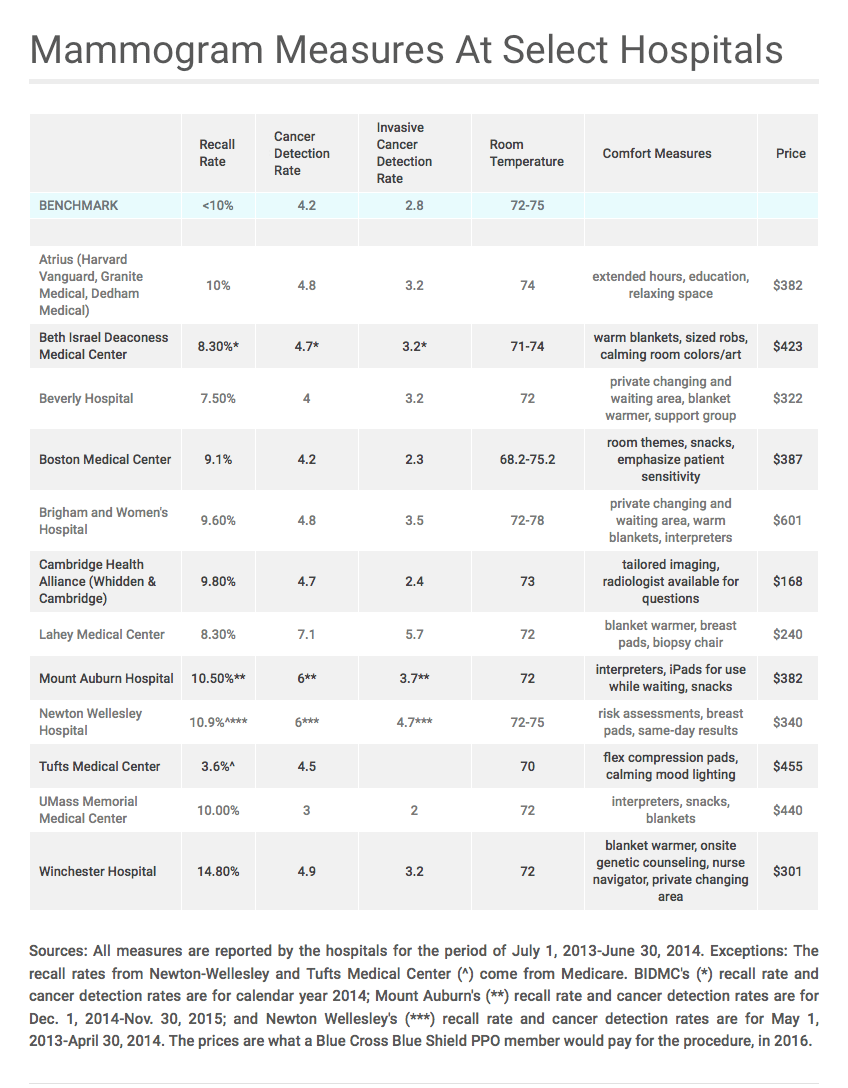
The table below (click to enlarge it) includes five ways you can compare quality across hospitals — and gives you a price. Explanations and details for each measure follow below the table.
As you review the table, consider three things:
- How does the hospital compare to the national benchmark for each rate?
- What factors might affect that hospital’s rate? We offer guidance below.
- How do the measures overlap?
“There’s a balance between low and high rates,” said Diana Miglioretti, a biostatistics professor at UC Davis School of Medicine and co-leader of the Breast Cancer Surveillance Consortium (BCSC), a project of the National Cancer Institute. She and other experts reviewed the mammography quality measures we're using.
Miglioretti suggests balancing the recall rate, which measures how often women are called back for more tests, against the cancer detection rate.
A recall rate below the national benchmark of 10 percent (as of 2009, the most recent data available) and a high cancer detection rate would be a good combination. It would mean that hospitals are finding cancer at an acceptable or expected rate without asking too many women to have unnecessary additional tests.
A high recall rate might also make sense if the cancer detection rate is high. That combination might mean that the hospital serves a lot of women at higher risk for cancer.
We have a lot more information about how to look for quality in a mammogram using the table (click to enlarge it) and the explanations below.
This is not a story about whether to get a mammogram, at what age or how often. You can read more about the latest recommendations here. We are not weighing the value of a routine 2D vs. 3D mammogram; the quality benchmarks we cite do not distinguish between the two tests.
But if you plan to get a mammogram, be aware: The cost and quality are different from one hospital to another.
Let us know if there are measures you’d like to see us add or subtract -- or if there are hospitals you’d like to include in the chart. We look forward to your feedback.
Recall Rate
What is this? The recall rate shows you how often a woman is told that she needs more tests based on something the radiologist saw on her screening mammogram.
The U.S. government posts recall rates for Medicare patients. The hospitals' rates on the table above are for all patients, except where noted.
Why does it matter? An unusually low recall rate may mean the hospital serves a relatively low-risk population — or that radiologists are missing signs of cancer. An unusually high recall rate may lead to unnecessary stress, costs and radiation from tests a woman does not need.
What is the benchmark? The recall rate benchmark is about 10 percent, as established by the BCSC. Recall rates of between 5 and 12 percent are considered acceptable by the American College of Radiology (see page 29 of this document).
What factors might affect the number? Hospitals that serve a high percentage of at-risk women or women having their first screening mammogram will have higher recall rates.
The recall rate may be lower at hospitals that use newer 3D mammography, rather than 2D tests.
And recall rates may be higher or lower based on the radiologist’s professional experience, his or her personality or the expectations of the hospital. Eighty percent of radiologists in the U.S. have recall rates between 4.6 and 15.7 percent, according the most recent data.
How should you use this measure? Mammography experts — like UC Davis' Miglioretti, above — suggest looking at the recall rate and the cancer detection rate together. Many radiologists say a relatively low recall rate is fine as long as the cancer detection rate (CDR) meets or exceeds the national benchmark. A high recall rate may be warranted if the CDR is also high.
Cancer Detection Rate (CDR)
What is this? A mammogram is a test that looks for cancer. This rate tells you how often radiologists at each hospital or clinic find cancer.
If you want a more technical answer... we asked hospitals to submit a rate using the definition established by the National Mammography Database (NMD): the number, per 1,000, of screening mammograms with a BI-RADS assessment category of 0, 4 or 5 that had a tissue diagnosis of cancer within 12 months.
Why does it matter? This measure tells you how often radiologists find cancer in the breast.
What is the benchmark? The benchmark, established by the BCSC, is 4.3 per 1,000. The American College of Radiology says a cancer detection rate of 2.5 per 1,000 or higher is acceptable. Eighty percent of radiologists have a cancer detection rate between 2.1 and 6.6.
What factors might affect the number? A high rate suggests a stronger likelihood of detecting the cancer, but doesn’t necessarily mean the hospital is better at detecting cancer. For instance: Hospitals that use 3D mammography may have higher cancer detection rates. Or the rate may be higher because a hospital sees more women at high risk for breast cancer.
How should you use this measure? “You want a high cancer detection rate,” Miglioretti, of UC Davis, said. “Where it’s too low, radiologists are probably not recalling enough women or not finding enough cancer.”
But Miglioretti says there are exceptions. If a hospital serves more low-income women who don’t have regular mammograms, they will likely have a higher cancer rate, but not necessarily because the radiologists are really good at detecting cancer.
On the other hand, if a hospital serves mostly women who are screened regularly, that hospital may have a low rate because problems were detected before they developed.
Invasive Cancer Detection Rate (ICDR)
What is this? Invasive cancer refers to cancer that has spread beyond a milk-producing gland or duct, where most breast cancer starts, and into normal tissue.
If you want a more technical answer… we asked hospitals to submit a rate using the definition established by the NMD: the number of screening mammograms, per 1,000, with a BI-RADS assessment category of 0, 4 or 5 that had a tissue diagnosis of invasive cancer within 12 months.
Why does it matter? "The ICDR is a bit of a proxy for, are we finding the cancers that matter?" said Dr. Janie Lee, director of breast imaging at the Seattle Cancer Care Alliance. If the cancer is invasive, it has spread beyond the ducts and "has the potential to spread elsewhere in the body."
What is the benchmark? There is no benchmark for this rate, but you can compare hospitals in Massachusetts against the rate for all hospitals that report to the National Mammography Database, which is 2.8 per 1,000, as reported by the NMD (page 9) for June 2013-June 2014.
What factors might affect the number? Hospitals or physician groups that detect more invasive cancer than the national rate may be doing a better job, or they may have more patients at risk for breast cancer. Hospitals that use 3D mammography may have higher cancer detection rates.
How should you use this measure? Mammography experts suggest looking at this as a subset of the overall cancer detection rate. So weigh the recall rate against the cancer detection rate, then look at the invasive number as a way to refine your assessment of the hospital. As with the CDR, a high invasive CDR is generally good. Keep in mind that the population a hospital serves may affect its cancer detection rate, as Miglioretti describes, above, in discussing that rate.
Exam Room Temperatures
What is this? This is the hospital-reported temperature or temperature range in the room where women have a mammogram.
Why does it matter? Women often complain that exam rooms are too cold, which makes it hard to relax. When a woman is relaxed, there is more breast tissue to place on the mammography plate and screen.
What factors might affect the number? Hospitals say they keep the temperature low in exam rooms to protect the mammography equipment, but they say they raise it as much as possible to keep women comfortable.
How should you use this measure? If being cold makes it difficult for you to relax, you might ask the hospital or clinic if they can provide a warmed blanket, or you could take other steps to help avoid tensing up with the cold.
Who sets the benchmark? We called some of the leading machine manufacturers and asked: How cold does the room need to be? The machines can operate within a wide range of temperatures: 68 to 86 degrees. The optimal temperature is between 72 and 76.
Comfort Measures
What is this? Many women say this test is uncomfortable or makes them feel anxious. We asked hospitals to list the steps they take to make the experience more pleasant and less anxiety producing. (In addition to the brief comfort measures in the table, see our longer post here.)
Why does it matter? Women who are uncomfortable or anxious are less likely to have regular mammograms.
What factors might affect the measures? Hospitals and clinics have different cultures or personalities that you may see reflected in their approach to patients and this test.
How should you use these measures? If you have suggestions for steps a hospital or clinic could take to improve your comfort, tell them.
Who sets the benchmark? You do.
Price
Why does it matter? The Affordable Care Act says insurers must pay the full price of a mammogram because it is a preventive test.
But there are at least three reasons to pay attention to the price. First, if you are called back for a second test, the first one may be labeled diagnostic, not prevention, and you'll be charged as you would for any other service. Second, your insurance company still pays, so spending more than needed will affect your insurance premiums in the long run. And third, balancing cost and quality will help you chose the best value test, even if you're not on hook for the price right away.
What is this? We've listed the price of a 2D mammogram at each hospital. This is the price Blue Cross Blue Shield of Massachusetts, the state’s largest insurer, would pay for a member who has a PPO plan. There is no uniform price for a mammogram. Each health plan negotiates a price with each clinic and hospital.
Some hospitals offer 3D mammography. Some, but not all, insurers cover the test. (A note for consumers: A few hospitals that offer the test say they bill for a 2D mammogram and absorb the additional cost if a patient's plan does not pay for 3D mammography. If you have a high-deductible plan or intend to pay cash for this test, you might want to get a cost estimate in writing in advance.)
What factors might affect the number? Some hospitals in Massachusetts use their market clout to demand higher rates, according to reports from the state attorney general.
Who sets the benchmark? There is no uniform or recommended price for a mammogram.
