Support WBUR
Commentary
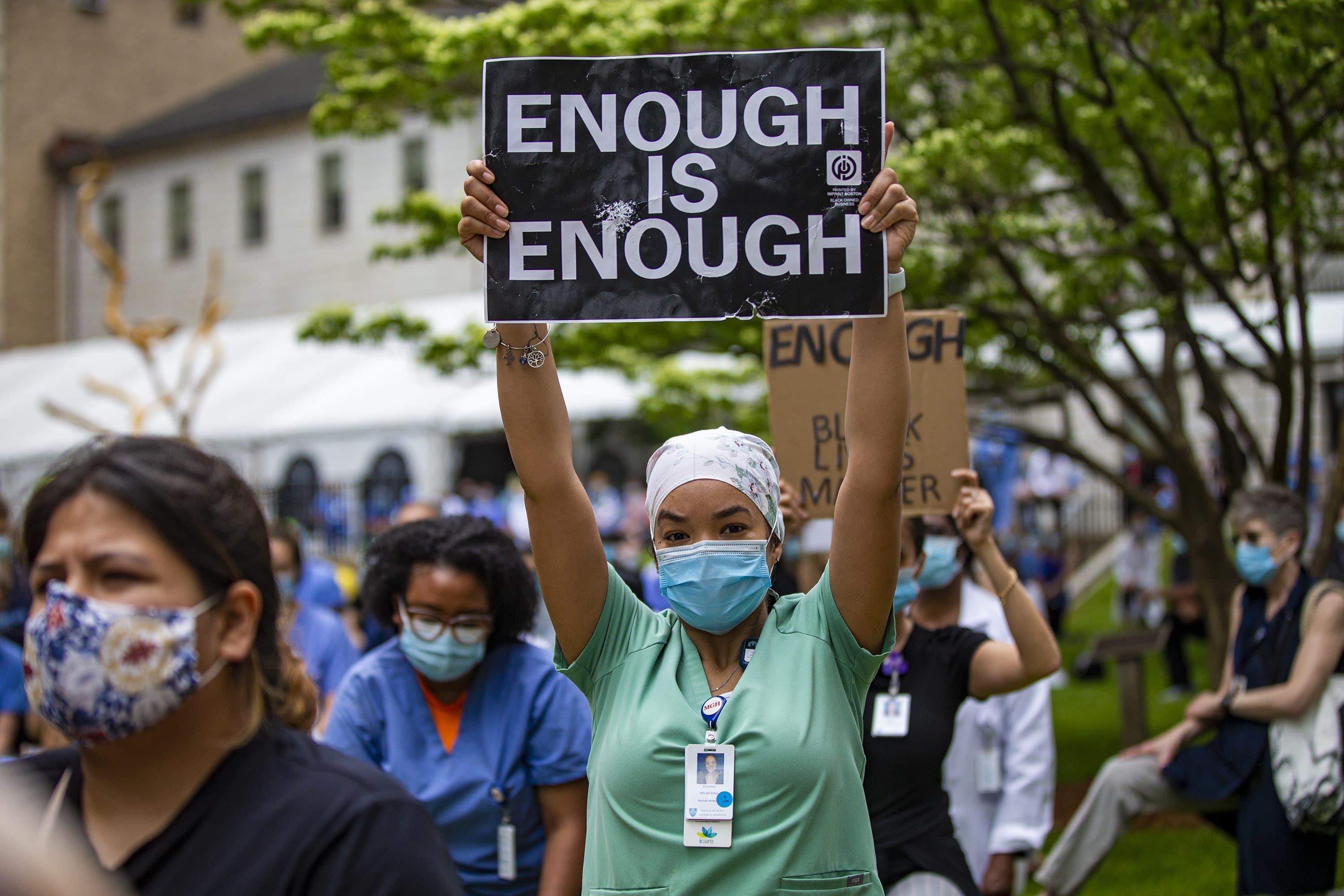
Racism In Medicine Isn't An Abstract Notion. It's Happening All Around Us, Every Day
Ahmaud Arbery. Breonna Taylor. George Floyd. Tony McDade.
For some, their killings illuminate racism’s stronghold on our society for the first time. However, police brutality is part of the epidemic of anti-Black racism initiated when the first slave ships docked on American shores in 1619.
Racism is part of my daily experience, even as a medical student rotating through the teaching hospitals of Harvard Medical School. The health care system is one sector within the larger framework of white supremacy embedded in American society. While the medical community accepts how the social determinants of health contribute to disparities, we hesitate to address how structural and interpersonal racism shorten Black people’s lives. Medicine has yet to actively become anti-racist.
Our non-Black colleagues must join in the fight for justice to relieve the disproportionate burden on Black physicians.
One experience, in particular, stands out.
As a second-year medical student, I attended a multidisciplinary meeting about whether a young Black woman admitted for a manic episode should be placed in the locked area of the unit. She had been walking around the unit wearing face paint resembling tribal markings and rapping the lyrics to music about being Black in America. On that basis alone, the floor nurses deemed this 140-pound woman a threat. At the back of the room, I had an internal debate about whether to speak up and note that wearing face paint or rapping is her expression of culture that reflects identity, and not threat. Throughout that meeting, every comment failed to acknowledge the room's overwhelming whiteness and the role structural racism played in this patient’s mental health and medical care. Eventually, I asked why we did not acknowledge the oppression she faces as a Black woman and explore her resilience. I was simply told she was too sick to engage in that dialogue. Following the larger meeting, I met with my resident for a debrief. He stated the normally unspoken, but widely accepted truth that on that particular unit, the darker someone's skin, the lower the threshold to restrain the patient.
The medical community largely avoids talking about how systemic racism affects our Black and brown patients individually. We are more comfortable talking about the social determinants of health for marginalized people, collectively, rather than discussing how we disenfranchise the patient under our care. Often, the few minority trainees and providers hold the burden of addressing these issues; they are constantly tasked to speak up for themselves and their communities.
As a Black woman, I am overwhelmed by wearing the hats of cultural mediator and trainee. We are forced to balance providing clinical care while witnessing the discrimination of our patients and ourselves. Additionally, we are asked to address and resolve these issues in a collective manner. The roles of colleague and patient advocate are often at odds as I strive to build strong team relationships but, more importantly, advocate for equity.
It is vital to educate everyone on a clinical team about the power of their implicit bias and micro-aggressions that demean their colleagues and offer disparate patient care. Medical education must equip trainees to interrogate health inequity with a critical race theory framework. Our non-Black colleagues must join in the fight for justice to relieve the disproportionate burden on Black physicians.
Ultimately, that patient was restricted to the locked area of the unit. During a subsequent interaction, she called 911 on her medical team and refused to hang up the phone and return to her room. Because of this, hospital security was called, and they carried her back to her room while she screamed that they should not touch her.
Just one week earlier, a tall elderly white man assaulted three different staff members before being moved to a locked room; security was not called until the third incident.
The stark contrast in their treatment emphasizes how threat is also racialized in our healthcare institutions.
Black women are three to four times more likely to die due to pregnancy-related causes than white women. Police killings of unarmed Black Americans cause 55 million excess poor mental health days per year among Black American adults, and from 2015 to 2016, on average 286.5 Black boys and men were killed by the police in the United States. Together, they lost 15,673.7 years of life.
It is time to start naming racism, and not race, as a risk factor for disease.
This is a call for the medical community to become actively anti-racist. Health care leaders must acknowledge police violence towards the Black community, and other manifestations of racism, as a public health crisis and implore our public systems for justice. We must take responsibility to address the inequities that shorten Black men and women’s life expectancy. We must reckon with medicine’s history of racism and structural violence. We must reevaluate our medical guidelines and institutional protocols to pinpoint "How is racism operating here?" and propose solutions as it is identified.
It is time to start naming racism, and not race, as a risk factor for disease.
Desmond Tutu famously said, “If you are neutral in situations of injustice, you have chosen the side of the oppressor.” As a medical community, we face an urgent decision to either speak out and break the stronghold of racial injustices or remain silent and tighten its bondage.
