Support WBUR
Commentary
Tuberculosis doesn't respect borders

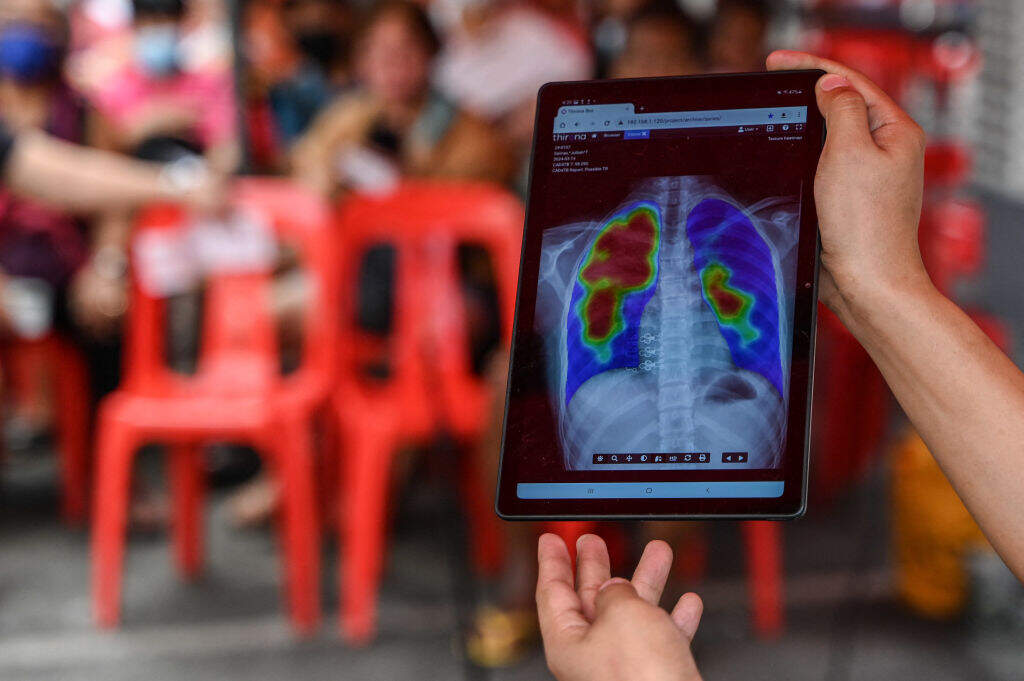
A patient we'll call Juliet is a young woman you wouldn't have noticed if you had happened upon her in the market or on a bus in the African country where she lived. She looks healthy. But she isn’t. As specialists in drug-resistant tuberculosis (DR-TB), we saw her at our clinic because her treatment wasn’t working. We were shocked to see how many drugs were resistant in the bacilli Juliet was coughing up. Out of more than 20 drugs we tested, only a handful were effective against the particular strain Juliet had.
TB is caused by a microorganism transmitted by the air from person to person. Active TB slowly destroys the lungs, causing patients to suffocate from oxygen starvation or blood in the airways. Some people call it the “contagious cancer” — it can often be cured if caught early and treated with months of chemotherapy. Unfortunately, TB can easily develop drug resistance — especially if the six-month course of antibiotics is paused or stopped — which makes treatment much more difficult and complicated. But Juliet's strain was one of the most resistant we had seen, so we recommended hospitalizing her in our specialized facility for DR-TB. She ended up staying for six months.
TB is the deadliest infectious disease in the world, killing more each year than HIV and malaria combined. Over the past few years, new TB drugs have finally made it through the long development process and transformed the treatment of DR-TB throughout the world, even in poor countries where patients like Juliet live. In the countries where we work, patients are overjoyed to receive these new TB drugs. But to our shock and dismay, even as these new drugs offer fresh hope, we are beginning to see patients like Juliet who are resistant to even the latest TB drugs.
From its peak in the 19th century, when it was known as the "White Death," cases of TB declined steadily in the U.S. and Europe, thanks to better nutrition, less crowded living conditions and the invention of antibiotics. In the rest of the world, however, TB has continued to run rampant. About 1.3 million people die from TB each year, despite the existence of highly effective antibiotics. Drug-resistant strains inevitably pop up wherever conditions prevent patients from taking complete courses of treatment, for example when economic crises or war cause health systems to collapse. In some countries in Eastern Europe and Central Asia, more than 20% of all TB is drug resistant.
Unfortunately, DR-TB doesn’t respect borders. A cough in a minibus in Maputo will eventually affect a schoolchild in Minnesota. So the only way to stop the spread of DR-TB is to treat one patient at a time in the faraway communities and countries where it thrives.
Until a few months ago, USAID was arguably the most important donor in the fight against TB. USAID funding was instrumental in the development of new TB drugs and diagnostics that helped doctors keep one step ahead of the TB bacilli. Even more important, USAID-supported hospitals and health centers detected and treated TB in the 24 countries with the highest TB burden. This direct, life-saving support to patients has been cut almost completely. Even the one global project specifically focused on diagnosing and treating DR-TB, Global Resilience Against Drug-Resistant TB (GRAD-TB), has been terminated.
Unfortunately, U.S. funding for global TB control — including prevention and treatment of DR-TB — has almost been completely shut off, which means that DR-TB will continue to grow and make the world a more dangerous place for us all.
DR-TB often has a profound physical and social impact on the lives of patients like Juliet. Even before coming to our clinic, Juliet had struggled physically and economically for years —first with HIV, and then with TB. After a diagnosis of extensively drug-resistant TB (XDR-TB), she received a complex cocktail of medications with noxious potential side effects, including nausea, vomiting, nerve pain and hearing loss. During the six months she was hospitalized, she saw her young daughter only during occasional visits and was unable to work to provide for her family.

In countries where we work, the health care systems are more rickety than most Americans can imagine, and poorly equipped to address a complicated disease like DR-TB. In many countries, the government health budget is less than $30 per person per year, which barely covers health worker salaries and a few of the cheapest medicines. Without foreign aid, the type of drugs and economic support that Juliet received is well beyond the capacity of most health systems in poor countries. And even with this care, Juliet's 18-month treatment course was difficult. She survived, but suffered permanent hearing loss and her daughter became infected with DR-TB.
There are thousands of patients all over the world like Juliet, mostly undiagnosed and expelling millions of bacilli into the air with every cough. The solution isn’t mysterious. We need to immediately restore U.S. funding to fight DR-TB. That includes direct support for DR-TB treatment programs, research in new diagnostics and drugs and renewed surveillance to catch resistance before it spreads.
Our public health shortsightedness will create thousands of highly resistant strains that will infect patients for decades. Stopping the fight against DR-TB today, even temporarily, will have irreversible, catastrophic effects in the long run — for generations to come.
Follow Cognoscenti on Facebook and Instagram. And sign up for our weekly newsletter.