Support WBUR
Another Suspected Ebola Case In Boston: 5 Reassuring Thoughts
This morning, my heart went out to WBUR's Jack Lepiarz as he waited outside Massachusetts General Hospital in the pre-dawn rain, shivering despite his five layers of clothing, for possible word on a patient who may have Ebola.
But along with my sympathy, I felt an odd calm — very different from the alarm I felt in mid-October when we had an Ebola scare in Braintree.
What's changed? Perhaps more than anything, the steady accumulation of time without another case contracted in the United States since two Dallas nurses caught the virus from Thomas Eric Duncan eight weeks ago. But also, it's that this rare and terrifying virus, synonymous with "Hot Zone" nightmares, has become ever more familiar, and its limits more clear — even as it remains a major scourge in Africa.
The latest word from MGH is that the patient's initial test for Ebola was negative. Good news, but these are the thoughts that most suppress my stress hormones:
1. Boston Hospital Strong
This is the medical mecca that became a model for the country in its handling of the marathon bombing injuries. It was prepared for that emergency, and, as Martha Bebinger reported, it has six hospitals prepped and ready for Ebola patients:
The six hospitals collaborating to provide care include Bay State Medical Center in Springfield and five Boston facilities: Boston Medical Center, Beth Israel Deaconess Medical Center, Brigham and Women’s Hospital, Tufts Medical Center and Massachusetts General Hospital.
“Hundreds of people at each hospital have spent incalculable hours in the necessary planning, training and practice efforts that are needed to respond to the challenges posed by this disease,” said Dr. Paul Biddinger, vice chair of emergency preparedness at Mass General.
Boston Children’s Hospital says it expects to join the Ebola treatment collaborative, and UMass Memorial in Worcester may as well. The other 59 acute care hospitals in Massachusetts would screen a patient, hold anyone who is at high risk or Ebola-positive in isolation, and then transfer the patient, says Public Health Commissioner Cheryl Bartlett.
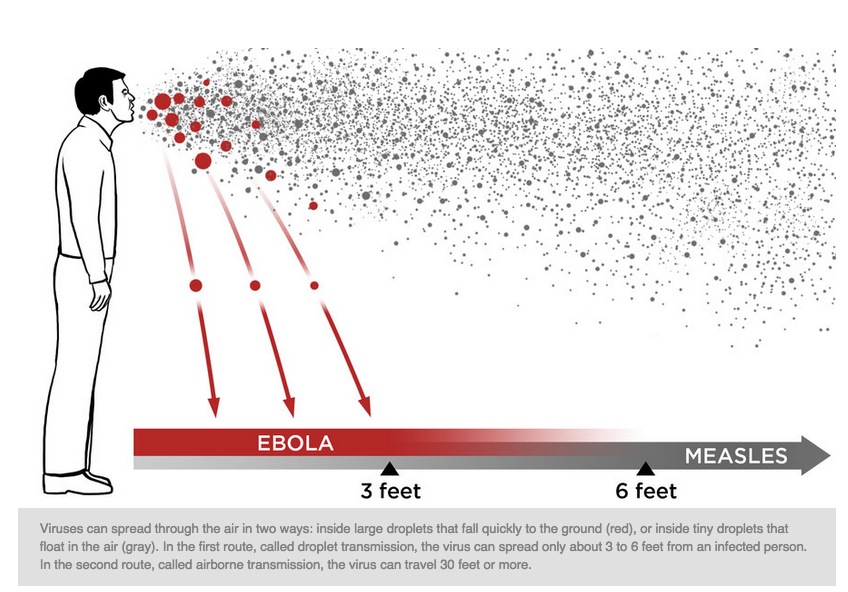
2. Airborne? Not
Scientists don't like to say "never," so even though all indications are that Ebola spreads only through direct contact with bodily fluids, it initially scared me when there were even hints that it might spread more easily.
This interview with Boston University Ebola researcher Elke Muhlberger helped — Reality Check: How People Catch Ebola, And How They Don't -- but what helped even more was this great recent explainer from NPR: Ebola in the Air: What Science Says About How Ebola Spreads.
It includes the helpful graphic at the top of this post, and this wonderful little story, to be recalled when next you sit near a coughing passenger on the T:
Take the case of Patrick Sawyer. Back in July, the Liberian-American businessman boarded a plane from Monrovia to Lagos, Nigeria. He was clearly very sick — and very contagious — with Ebola. He even vomited while on the plane.
There were about 200 other passengers on the flight. None of them got infected.
3. Bedside Care
Ebola is a death sentence. That was my impression as it began to sweep through Liberia and Sierra Leone. But then a few lucky foreign patients got their medical care in high-tech Western hospitals, and most survived. The New England Journal of Medicine described the treatment of two Ebola patients who survived with fluids and electrolytes, among other supports. Dr. Paul Farmer of Partners In Health fame wrote:
…the fact is that weak health systems, not unprecedented virulence or a previously unknown mode of transmission, are to blame for Ebola’s rapid spread. Weak health systems are also to blame for the high case-fatality rates in the current pandemic, which is caused by the Zaire strain of the virus.
The obverse of this fact – and it is a fact – is the welcome news that the spread of the disease can be stopped by linking better infection control (to protect the uninfected) to improved clinical care (to save the afflicted).
An Ebola diagnosis need not be a death sentence. Here’s my assertion as an infectious disease specialist: if patients are promptly diagnosed and receive aggressive supportive care – including fluid resuscitation, electrolyte replacement and blood products – the great majority, as many as 90 per cent, should survive.
4. Practice, practice, practice
We don't hear about every suspected case of Ebola in Massachusetts, but there have clearly been others, and there will be more. And each false alarm is a chance for more instructive practice that can cut the confusion if the crisis is real.
The CDC has refined some of its guidelines for handling potential Ebola patients, and Dr. Ben Kruskal, chief of infectious disease at Harvard Vanguard Medical Associates, notes that the many protocols needed for managing potential Ebola patients must all be in place beforehand, and staff must be trained in them.
Among the lessons he sees from the Braintree incident: Coordination can be a challenge when suddenly public agencies at the town, state and national levels are all involved, from the local police to the CDC.
5. Our Local Gene Masters
True, this one is a bit more obscure, but should we need to sequence the genes of an Ebola virus found in a Boston patient, hey, we can do it locally — and thus quickly.
The Broad Institute, the genomics powerhouse in Cambridge, houses a gene sequencing center just described in The New York Times as "the world’s most powerful factory for analyzing genes from people and viruses."
Among Broad researchers on the case is Dr. Pardis Sabeti, an award-winning computational geneticist who has mapped mutations of the Ebola virus. (She's also musical. See: Why Are These Scientists Singing About Ebola?)
Readers, did you, too, find that this latest case of suspected Ebola struck you differently this time? How?
