Support WBUR
Is animal testing even needed anymore?
For almost 90 years, the U.S. Food and Drug Administration has required all new drugs to be tested on animals prior to federal approval.
But now, some computers can accurately model human body systems, and miniature organs can be grown on chips.
Today, On Point: Is animal testing becoming obsolete?
Guest
Dr. Donald Ingber, founding director of the Wyss Institute for Biologically Inspired Engineering at Harvard University. Founder of Emulate, Inc., a leading manufacturer of organ-on-chip systems.
Also Featured
Birgit Girshick, Chief Operating Officer of Charles River Laboratories.
Nicole Kleinstreuer, Acting Deputy Director for Program Coordination, Planning and Strategic Initiatives at the National Institutes of Health.
Dr. Jenny Tam, Director of Synthetic Biology at the Wyss Institute for Biologically Inspired Engineering at Harvard University.
Transcript
Part I
MEGHNA CHAKRABARTI: In the 1930s, the S.E. Massengill Company of Bristol, Tennessee had a problem. They wanted to convert a pill into a liquid, and they wanted to market that liquid as an elixir. Now, the pill was sulfanilamide, an active ingredient that fought streptococcal infections. The liquid would make it easier to ingest.
The only problem? It tasted terrible. So the company added a bunch of stuff to make it more palatable. Things like raspberry extract, saccharine, and another sweet-tasting solvent called diethylene glycol.
Now, there's a good chance that you've smelled diethylene glycol before because it's more commonly known as antifreeze.
Well, this elixir went on to kill more than 100 people, including more than 30 children. And that disaster led to a pivotal law passed in this country in 1938, one that has stood unchallenged for more than 80 years until 2022.
SEN. RAND PAUL [Tape]: Mr. President, I rise today to talk about a bill that would lift a mandate in the law dating back to the Great Depression.
CHAKRABARTI: So that was Kentucky Sen. Republican Rand Paul in September of 2022, testifying in favor of the FDA Modernization Act 2.0. Now, the specific mandate Sen. Paul is referencing there is to the 1938 requirement that all new drugs be tested on animals for safety before they move on to clinical trials.
The FDA Modernization Act 2.0 is the first major step that could bring an end to pharmaceutical animal testing. It authorizes FDA to accept alternatives to animal testing that have been developed in the past 50 years, things like computer modeling and stem cell research.
SEN. PAUL: It's often said that the definition of insanity is doing the same thing over and over again and expecting a different result. We've mandated animal testing for the last 84 years. And it meant slower approval for promising drugs and cures. The time has come for the law to finally catch up with the science.
CHAKRABARTI: President Joe Biden signed the act into law three months later in 2022.
Well, earlier this year, FDA officially announced that it's phasing out animal testing requirements for some therapies and drugs in favor of more effective, human relevant methods, as it says. FDA commissioner Dr. Martin Makary spoke on the Megyn Kelly Show on April 17.
DR. MARTIN MAKARY: So these new technologies have the promise of replacing some of this routine animal testing. You would cut six months out of that approval process. You lower R&D costs for pharma companies and inventors, which could lower drug prices for everyday Americans.
CHAKRABARTI: Well, today we're going to further explore whether animal testing is becoming obsolete in the development of new pharmaceuticals. And, if so, how to ensure that technological replacements are as safe or actually even safer in modern day drug development as that development becomes more personalized and sophisticated.
Well, Dr. Donald Ingber is founder of the Wyss Institute for Biologically Inspired Engineering at Harvard University. He's also founder of Emulate, a company that's a leading manufacturer of what's known as organ-on-ship systems.
Dr. Ingber, welcome to On Point.
DR. DONALD INGBER: Thank you. It's my pleasure.
CHAKRABARTI: Okay. First of all, let's talk specifically about what FDA has announced, because I wanna get your understanding as to how much of drug development this actually covers because it's specific to monoclonal antibody therapies.
INGBER: It's actually not specific. It's saying that's where they're gonna start.
CHAKRABARTI: That's where they're gonna start. Okay.
INGBER: But since the Modernization Act 2.0 in December 2022, they have stated that they are open to reviewing investigational new drug applications — which is what pharmaceutical companies submit to get drugs approved — that include data from alternative models, including organs on chips, in lieu of animal data.
So they've been open for a while. But what this does that's different is that it really saying they're making it a priority and also there're incentives there in that they'll give accelerated reviews and try to accelerate the process if applications include data from these alternative models. And that's a game changer, I think.
CHAKRABARTI: Okay. So we'll come back to that. But help me understand specifically, what is mono — again, as the starting point for phasing out animal testing, what are monoclonal antibody therapies?
INGBER: Yeah, so most drugs that we've known are, you know, since we grew up with are small chemicals. They're very, very tiny. Monoclonal antibodies are engineered antibodies, just like we make antibodies to fight off infections. But scientists have developed ways to engineer them so they could target specific molecules on cells that, you know, for example, a pathogen or something that's involved in mediating inflammation, let's say an inflammatory bowel disease.
They are larger and they have different types of toxicities. Some are so specific for human targets that they can't cross-react with animals.
CHAKRABARTI: Uh-huh.
INGBER: So they have to use non-human primates and even sometimes non-human primates don't work for these highly specific therapies. And other therapies that you hear about, like CRISPR gene therapies, those are very human-specific as well.
CHAKRABARTI: Okay. So FDA has announced that AI-based computational models are under consideration, organoid toxicity models and testing. So we'll talk about all of that.
But again, for background purposes, I mean obviously animal testing on things like cosmetics has not been required for a long time, right? And that's why we see on shampoo bottles and things, "not tested on animals." But tell me a little bit more about currently, what's sort of the typical process? When does animal testing come into the process of developing a new drug?
INGBER: Well, I mean, if you start in the beginning, you know, most research that leads to drug development is funded by the federal government, right?
CHAKRABARTI: Yeah.
INGBER: You know, NIH, FDA funds work. DARPA, ARPA-H, things like that. Those studies are largely mouse-based. Because people have developed ways to engineer mice so that they look like a little bit more like human diseases. And so that's the early stage.
But the drug companies, to bring a drug for FDA approval, usually have to test for toxicities in two different species, often rats and dogs. That's why you see pictures of beagles. For some reason, beagles were used a lot in the past. And then some monoclonal antibodies often have to go to non-human primates because of that targeting specificity.
CHAKRABARTI: Right. So it sounds like at multiple key points in the development of new therapies, I mean, animals, as the process is practiced thus far, animal testing is still essential.
INGBER: Oh, it's a central part of the whole business of science and, you know, medical science and drug development.
But let me say: FDA is primarily focused on toxicity. Drug companies also are looking for efficacy, new target discovery. And that is largely animal-based as well. It has been in the past. And this is a big place where human alternatives are, I think, gonna be enormously valuable and are beginning to be enormously valuable.
CHAKRABARTI: That is an important distinction. Okay. So FDA is looking like, will it hurt you? Will it make you sick?
INGBER: Right. Safety.
CHAKRABARTI: Yeah, safety. But does it actually work is a whole different --
INGBER: They're obviously interested in that. But that is really what the clinical trials are gonna demonstrate. And there has to be demonstration animal models before that. But before they ever go to the FDA, these drug companies have spent, you know, 10, 15 years, hundreds of millions, and a lot of that involves animal work as well.
CHAKRABARTI: Okay. So, let's talk now, we're gonna spend the rest of the hour now talking about what these new technologies are that could make animal testing in pharmaceutical development obsolete. I mentioned the phrase organ-on-a-chip. What is that?
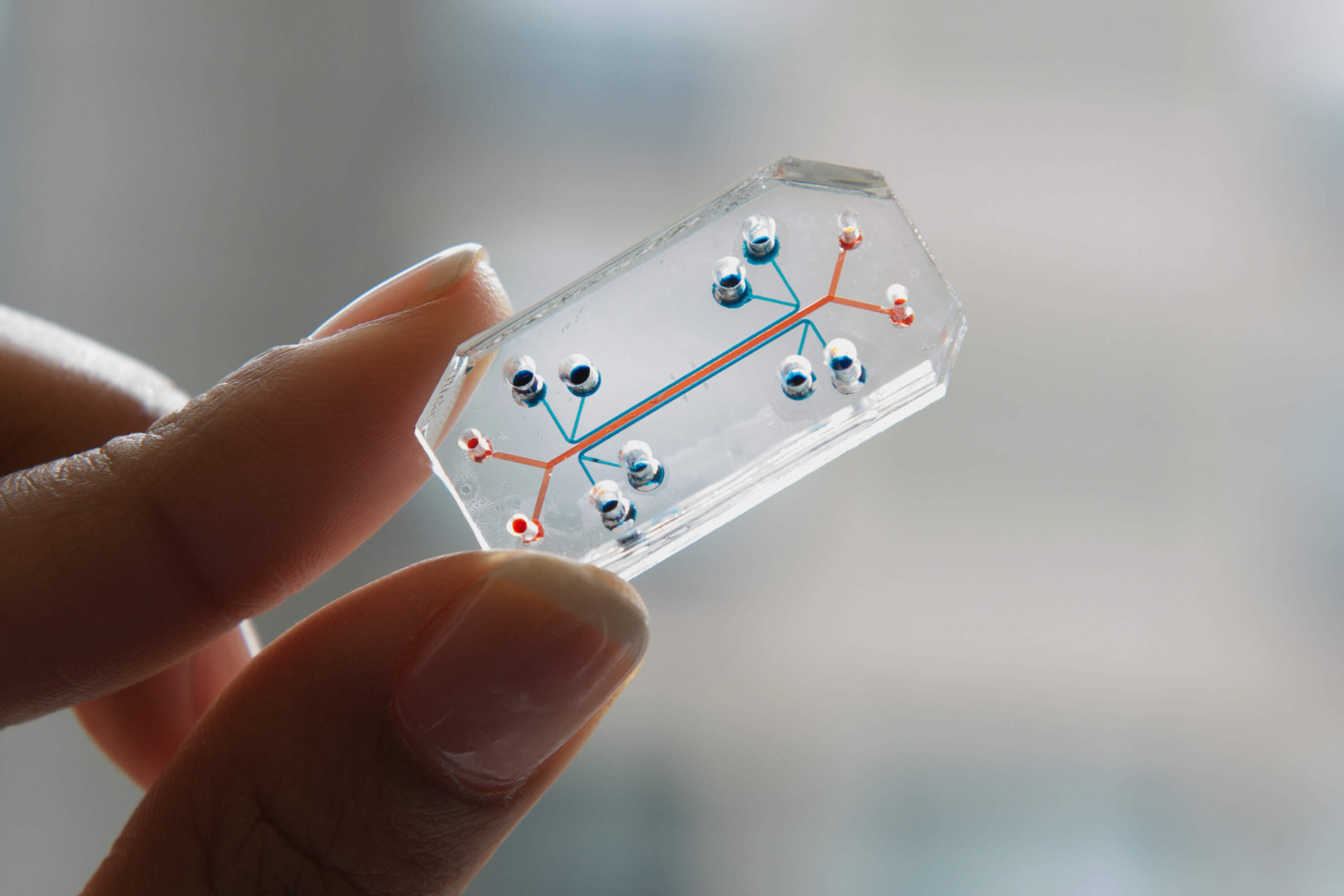
INGBER: So, organs on chips which we started developing, you know, 15, 20 years ago at this point, are small devices. They're size of a thumb drive or a computer memory stick, or old-school eraser. If you're old enough to remember those. You can hold them between two fingers. They're optically clear. They're made out of a flexible, rubber-like material.
"Organs-on chips ... are the size of a thumb drive or a computer memory stick."
But what we do is originally we called them chips because we use computer microchip manufacturing techniques to make them, because you have control over features at the same nanometer to micrometer, you know, incredibly small size that living cells and tissues live at.
So we make hollow channels less than a millimeter wide. We have two parallel to each other. You could think of them as you know, two tunnels you drive cars through. One goes one way, one goes the other. But we have holes in the wall between them, so we could put different tissue types on either side.
So in one channel, let's say the first chip, we put the lining cells of your lung air sac with air over them.
CHAKRABARTI: Mm-hmm.
INGBER: And on the channel below we put your capillary blood vessel cells with medium or we could even flow blood through them for short times as well.
CHAKRABARTI: So it's replicating the space where air from your lungs gets transferred into the blood.
INGBER: Exactly. And this is basically what makes we call it an organ on a chip, not a cell or tissue, because an organ are two or more tissues that come together, new functions emerge. Almost always you have to have a blood vessel because you need oxygen, nutrients, et cetera.
The other trick is that we developed ways to mechanically cyclically stretch these tissues. So we mimic breathing in the lung as well.
Now we do the same, we use the same chip with intestine and we put intestinal lining cells like, say, your colon on one side and your blood vessel cells or your connective tissue cells, and we mimic peristaltic motions. In the kidney, we can mimic the way the kidney glomerulus, where you have blood filtration into urine, every heartbeat stretches with the pulse of the blood. And we mimic that on this.
And because we mimic the chemical environment, the physical environment, and these 3D tissue-tissue structures or interfaces, we get recapitulation of the function or physiology of your organs and disease states at a level really never seen before, and it's all human.
"We mimic the chemical environment, the physical environment, and these 3D tissue-tissue structures ... [and] we get recapitulation of the function of your organs ... at a level really never seen before."
CHAKRABARTI: This is what answers the question that I had about the process. Because, you know, in my mind I thought, okay, well if it's just like cells, that's not the same thing as the function of an entire organ, right? But you're mimicking the function here. The structure and function at a microscopic level.
INGBER: And we have a window on the molecular activities in these cells while they're in this tissue organ context. Because it's optically clear, we could look under the microscope. We could collect the outflows. So we could take samples of the blood vessel channel, just like a doctor takes blood sample out of your vein. And we could use that to discover new biomarkers of disease or new clinical biomarkers of drug response.
We could collect the outflow of the intestinal lumen channel and we have biomarkers for stool samples. We also can grow microbiome. Which has been like one of the major changes since I went to med school, a paradigm shift that, you know, we never, we didn't learn about, but it's a major part of health and disease.
We can grow complex human micro — literally gut microbiome in intestine chip for extended time and see how it affects the host and vice versa.
Part II
CHAKRABARTI: And Dr. Ingber, you were describing to me what the organ on a chip system is. A little bit later we're gonna hear about something else called an organoid. That's another new technology or what are organoids?
INGBER: Yeah. It's another great technology. And I think it's one thing that's great about the FDA's announcement is that they're combining, they're exploring many different technologies.
Organoids are little balls of cells that you form by collecting a biopsy from an adult where you get stem cells. These are the cells that replenish your tissues, like your intestine turns over every three days. So there's cells in there that can keep forming all the specialized cells of your organs.
And so they would take a biopsy from a patient, for example, you collect these stem cells, you grow them in a Jell-O like material, and they grow into a ball. And if it's an intestinal cell, they'll begin to form structures that look like your intestinal villi.
But these are more, I call them tissue-oids in general because it's one tissue type. They don't have the blood vessels. They don't have the immune cells. They don't have the connective tissue. You also can make them by using a technique called induced pluripotent stem cells, IPS, which basically is take a cell from your blood, a cell from your skin connective tissue, you throw in a few genes and chemicals, and you make an embryonic stem cell-like cell that can form almost any tissue type in your body.
And so people are using that, for example, for brain. And there you get many different types of brain cells, which is quite interesting. And if you go long enough, they begin to form interesting multicellular structures. But again, they lack — the difference about organs-on-chips is that we actually use organoids as a source of cells.
CHAKRABARTI: Mm.
INGBER: We grow them in the gel. But then we break them up, put them on one channel, and we interface them with the other tissue types that they see in the body. And we could have flow and air and peristalsis and breathing.
And what's important about that is we can mimic the way drugs actually change their levels over time in the body. It's called pharmacokinetics. You know, your doctor will prescribe a drug once a day or three times a day, or you go to the hospital, you get a continuous infusion. That's because the same drug at a totally different dose or timing will give you --
CHAKRABARTI: Different results.
INGBER: Different results, toxicity, I mean, aspirin can kill you, obviously, right? So we can mimic precisely the dose changes over time because we have flow.
CHAKRABARTI: And is the idea that ultimately — because you talked about taking samples from a patient — that you would even find out specifically the response that that specific patient would have?
INGBER: Absolutely. We just published a paper with a collaborator at McGill a surgeon, Lorenzo Ferri, and he had patients with esophageal cancer. And they get resistant to therapy. And basically, you don't know which therapy to try next.
He's made these chips with their cells and he flows in the drugs — the various ones that he's choosing between, at doses they would see in the patient — through the channel that's analogous to the blood vessel channel. The way they would see it, not just giving it to cells in a dish. And you actually can determine what drugs to give the patients.
They used organoids actually as a comparison, and because of this ability to mimic changes in drug exposure profiles, the chips were more effective than the organoids. However, they use both in combination because organoids are actually a higher throughput. You could do studies often faster with many different, you know, with many at a time.
So each one of these has power. And the organoids are, are very effective at modeling the cellular level response. These organs-on-chips kind of get you that higher level complexity. So we see them as partners in this whole thing.
CHAKRABARTI: Okay. So let's listen to Nicole Kleinstreuer. She's the acting director for program coordination at NIH. And she spoke with On Point and told us NIH is going to focus on increasing funding — I can't believe I just said that in these times — but NIH will focus, that's what they say.
INGBER: I'll believe it when I see it.
CHAKRABARTI: Yeah. On increasing funding and public awareness around alternatives to animal testing. And here's what she said:
NICOLE KLEINSTREUER: You know, we have no intention of just phasing out animal studies overnight. We know that animal studies are still very important and often scientifically justified. There are lots of areas where validated human-relevant models are not yet available. But we are seeing rapid progress and the more we invest in this space, the better those human biology-based integrated systems will become and the less we will have to rely on animal models moving forward.
CHAKRABARTI: Dr. Ingber, when she says there are lots of areas where validated human relevant models are not yet available, tell me more about that.
INGBER: Well, that's an important point. Because for the FDA, for example, they use the term qualify, and that means you have to show that one of these alternative systems replicates the normal function of an organ as well as can be as good or better than an animal model at predicting the response to drugs.
CHAKRABARTI: Right. You have to prove it. Yeah, exactly.
INGBER: So for example, Emulate, the company that you mentioned I founded is the farthest along in going through a program that FDA has called ISTAND, which if it gets through that successfully, the FDA will sort of certify it so that any company can use that model to replace, in this case, a liver toxicity model.
CHAKRABARTI: Mm-hmm.
INGBER: But that required Emulate to test 870 chips created with cells from three different human donors. And there's four different cell types to create this organ level structure in these chips. They tested 27 different drugs of which we already knew the results in rats and dogs and humans, of which many of these drugs were wrong because most times these animal models are wrong.
And we could show that this liver chip was about seven to eight times more effective at predicting the results in humans than the animals. Now, that has been in the ISTAND program, the first letter of intent was in the spring of 2022. And it's still going. Okay?
But so one thing is how quickly this will be done. But the other is every chip you have to — or organoid model or computer model — would have to go that sort of qualification. And this is where the real challenge lies. So it's not gonna happen overnight. But it's happening.
"This liver chip was about seven to eight times more effective at predicting the results in humans than the animals."
CHAKRABARTI: Yeah. But it makes a lot of sense though, right? Because if you don't validate these things, then it's just like, well, just another fancy toy. You want it to actually, like, predict what's going to happen to humans, like you said, better than animal testing.
INGBER: It's perfectly reasonable. But it has to be accelerated in terms of the pace.
CHAKRABARTI: Okay. Let me ask you one thing, because you talked about the original tissue for the organ on a chip or even organoids that's coming from humans. It's human tissue.
Now, in this day and age, anytime I hear that it's hard not to imagine that politics can creep in. Because, you know, for example, you said stem cells. And we know that you know, politics around abortion have of oftentimes sort of entered the space when it comes to stem cell research. Where are your — you talked about patient original samples, where are the other human tissue samples coming from?
INGBER: None of these are embryonic cells.
CHAKRABARTI: Okay.
INGBER: And these are usually coming from cadavers where people have agreed to donate their tissues. And, you know, companies sell them. Or surgical, a biopsy, you know, basically they're looking to see if you have a ulcerative colitis, but they take a sample, turns out to be normal. The patient has volunteered that it can be used. The induced pluripotent stem cells are again from patients who have volunteered to donors. So none of this is embryonic.
CHAKRABARTI: Okay. So let's go into a lab now. Because earlier this week, On Point producer Will Walkey visited Dr. Jenny Tam, director of the Wyss Institute’s Synthetic Biology platform in Boston, Massachusetts.
DR. JENNY TAM: So this is our stem cell culture room. We're very clean in here. We don't wanna get our stem cell cultures contaminated with anything, so we put our lab coats on and our gloves on to keep everything clean.
CHAKRABARTI: Dr. Tam's research includes screening drug treatments for bipolar disorder. And to do so, her lab uses organoids that we talked about a little earlier. So a lay person's way of describing them might be small, tiny balls of stem cells.
And at the lab, Dr. Tam obviously uses freezers to keep the cells at just the right temperature and robots to pipette small amounts of fluid onto the organoids.
TAM: There's like 96 wells in that plate, and you can see all these plates that need changing. They need to be fed. So if you kind of think of your child, and each well's a child, you need to feed all 96. (LAUGHS)
WILL WALKEY: What are you feeding them with?
TAM: So, so this is media, so they're just nutrients that helps your cells to grow. But there's a specific cocktail that's specific to these stem cell cultures.
CHAKRABARTI: It usually takes months, Dr. Tam says, but once the organoid grows, it can mimic even different parts of the brain. And I was curious about this: The final product does not just look like a miniature brain.
TAM: So you might say, how can you tell me what you're showing me is real? So this is an instrument, it's called a micro electrode array device. So there's like a little square with lots of — over 26,000 individual electrodes.
They place the organoids on top of each area of the micro electrode array. And those electrodes are so tiny that they can interact with different parts of the region of a single neuron. And so you can measure that neural activity across the cell and how that neuron interacts with other neurons inside that organoid.
CHAKRABARTI: So this is important because you only know for sure what you can measure. And in Tam's lab, they can compare drugs introduced to organoids grown from the stem cells of patients that have been diagnosed with bipolar disorder. And they compare those to those grown from a control group.
TAM: So we introduced this, the drugs in the media over a specific time point. And we have done that. And we have tested both lithium, which is a standard drug that's often used for treatment in bipolar. And really exciting: We discovered a new drug that has not been used in bipolar using our platform.
And so we have tested that drug on our organoids as well. And so we saw that the drug normalized that neural activity back to someone who has not had bipolar.
CHAKRABARTI: Dr. Tam has photos and videos of other types of organoids like livers, kidneys, and even beating hearts, which she showed to our producer.
And Tam says she got interested in bipolar research specifically because the disorder is so hard to treat. You heard her mention lithium there earlier — a very commonly used, but far from perfect therapy. Bipolar affects 40 to 60 million people worldwide, and on average it can take as much as eight years to even diagnose.
TAM: And then when you look at the cross-section of who is not diagnosed correctly, I mean it's just mind-boggling and heartbreaking. And that we can't get treatments to people quickly is terrible. I think it's a derelict of duty in some ways.
CHAKRABARTI: Tam also currently works with some lab animals. And she says overall, they're ineffective for bipolar disorder research.
TAM: So for mood disorders, it's hard to give a survey to a mouse to ask if you're feeling very depressed that day, or you're feeling hyper-excited that day. (LAUGHS) So we do like behavioral models.
So we measure how fast a mouse will be spinning on a wheel. We'll measure how much they'll move in inside of a cage. And then we — there are associated genes that are related to bipolar. Again, this is just a specific behavioral model. And then we'll knock out certain genes. Knocking that out means removing those certain genes that have been implicated in genetic studies towards bipolar.
So we'll knock out those genes and say, what does that affect? As we just discussed, there's multiple genes associated with bipolar disorder, so looking at one gene is not enough. It shows that it's one aspect, but it's a very slow way of doing that.
"It's hard to give a survey to a mouse to ask if you're feeling very depressed that day, or you're feeling hyper-excited that day."
CHAKRABARTI: Dr. Tam is hopeful that organoids can be a more useful test or system for drug development because they, again, use human cells — even as she acknowledges the technology's current limitations.
TAM: So as we kind of create different brain regions, we would like to merge these different brain regions into more complex model systems. I mean, right now that's, that is an advantage that the mice have over, you know, some of these in vitro models because they have the complete organ system. But that's — we're still working on those advances.
CHAKRABARTI: Dr. Ingber, in fact, a little bit earlier you talked about sort of what organoids do well and what organs on a chip do well. And you called them complementary. Listening to Dr. Tam's examples there from bipolar disorder research, it makes a lot of sense.
But, what do you think are still the major areas of advancement needed to make these technologies as effective as possible in drug development? Like, what do they not do that you'd like them to do?
INGBER: So, first I have to say, because I collaborate with Jenny, my team and her and the team she works with and George Church at the Wyss Institute is that it's a great example where AI actually compliments organoids as well as we've done this on organ chips. And that we've used AI-based computational approach to come up with the drugs that they're finding actually have activity in those organoids.
And the other thing is that in the organoids, they could visualize thousands of gene changes at once because you have this whole multicellular structure, where in the mouse they have to like knock out one at a time.
CHAKRABARTI: Mm-hmm.
INGBER: And you could see these drugs actually — for example, these bipolar patients have problems with circadian rhythm and sleeping at night, for example. You could see these organoids light up the brain cells light up activity in cyclical ways, normal, healthy brain organoids, but not in the bipolar. And you could kind of try to reverse that with drugs. So you can do levels of complex functionality and responses in these systems that's hard to do in mice.
"You can do levels of complex functionality and responses in these systems that's hard to do in mice."
CHAKRABARTI: But let me ask you, when we talk about toxicity, though, again, like if, again, if the, the organoids or the organ on a chip is sort of really focused on one one physiological system. What if there's a toxicity response in another organ system? Right?
INGBER: So, first of all. You know, early on I was funded by DARPA to create a human body on chips. Okay? So we were funded to create 10 different organs, which we did to link them together by their blood vessel line channels fluidically, meaning transfer fluid to the other and keep them alive for a month using an automated instrument.
We did that. That was the beginning of Emulate, effectively. But it's very hard to do because you have to get them all running one at a time. But you can actually do that, transfer fluids from one to the other to look at toxicities across the whole body.
Part III
CHAKRABARTI: Now, Dr. Ingber, if you just hang on for a few minutes here, we wanted to speak with someone who still believes that there is a place for animal testing when it comes to pharmaceuticals.
And for that, we spoke with someone at Charles River Laboratories. It's a pharma company based here in Boston as well. They had some $4 billion in revenue last year. Birgit Girshick is the company's Chief Operating Officer and she told us that animal breeding and testing is a major part of Charles River's business.
BIRGIT GIRSHICK: It's a core function of our company supported by many different in vitro technologies, mostly to assure patient safety. But also to provide early insights into a molecule and its suitability to become a drug product.
CHAKRABARTI: Not that FDA's announcement did not have an impact on Charles River Laboratories. The company's stock tumbled almost 30% the day after FDA's announcement. But Girshick says she actually welcomed the news.
GIRSHICK: It's a great signal to the world, to society, but also to us in the industry.
CHAKRABARTI: Because she sees FDA's announcement as validating work Charles River Laboratories is already doing.
Because in the world of animal testing, Girshick tells us that researchers abide by three Rs to reduce animal use in the name of science: Replacing animals when there are good alternatives, like organ on a chip; reducing the numbers of animals necessary for an experiment; and refining studies when animals are absolutely needed for testing.
So in some parts of their lab, Girshick says the number of lab animals has actually dropped by 50% over the past decade using those guidelines.
GIRSHICK: So we are currently doing a roughly $200 million of revenue using these technologies, so organoids, organ-on-chip, in silico, in all different areas. And they're used as part of the drug development continuum. They're used side by side with animal studies. And we believe that over time more and more hybrid studies will be run.
CHAKRABARTI: Okay. And that's exactly why she thinks that animal testing won't come to a complete end yet. Because as we've discussed before, there are hurdles such as modeling very complex systems and responses to a drug on an entire body.
GIRSHICK: The safety profile of many molecules are still not known. So there's a high risk that once this molecule, once this drug enters a body — and this would be the human body — you don't know what happens.
So you don't know if it's accumulating in the thyroid. And if you don't have a platform that can replicate a human body, which would be all 78 organs of a human body, you don't know what other side effects it could have.
"If you don't have a platform that can replicate ... all 78 organs of a human body, you don't know what other side effects it could have."
CHAKRABARTI: Girshick says the future for now is hybrid models — primary studies using organoids or organ on a chip, also AI, as we talked about earlier. But then coupled with smaller animal studies that could get new drugs to clinical trial faster. And ideally cheaper. But not jeopardizing patients.
GIRSHICK: A living body is not like anything else in the world. It's not a machine, it's not a computer, it's, it's reacting depending what, if you had enough sleep or not. If you're taking other drugs, how it's interacting. There's so many variables that you need to consider, and that's why so many drugs are failing, right? Because if it would be easy, we would all do it. And we would all do it today.
CHAKRABARTI: So Dr. Ingber, a few minutes ago you did acknowledge that it's really hard to model an entire human body, which is what Girshick is saying there. I mean, so what do you think about this idea of sort of hybrid testing regimes?
INGBER: I think that's exactly what's happening now and needs to happen right now, and we're not gonna get rid of animal studies right away.
I mean, there's things like, you know, cognitive disorders and schizophrenia and things like that that are, it is just very hard to model some of these things in vitro. But you can hear from Jenny Tam that you could start approaching some things that you'd never think possible before. I think --
CHAKRABARTI: Dr. Tam also said you can't do a mood survey on a mouse. (LAUGHS)
INGBER: Exactly right. I also wanna mention that, you know, yes, the whole human body is important, but AI can help with a lot of this. Because we know a lot of results. There are examples where drugs were totally toxic in animals and they weren't toxic in humans, we always worry about how many good drugs we lost because of that.
There's often failures in clinical trials because of comorbidities, meaning like a patient has three other disease processes. They're not healthy mice. We can model that in chips, for example, when we take a lung chip with cells from a patient that has chronic obstructive pulmonary disease, COPD, they're 10 times more sensitive to viral infection on chip, just like they are in real life.
So you, you could be testing for drugs and picking up complexities that come from other disease processes, which you don't — you can't really do in animals. I think the answer is it's gonna be these three Rs, like progressively replacing, reducing refining.
CHAKRABARTI: Yeah.
INGBER: And the FDA will only approve a replacement for a specific context of use. So for example, the liver chip that we're moving along to get approved to replace drug-induced liver injury is only with small molecule drugs. And it's only for liver injury. Now the speaker was right at Charles River that when you do — when you're testing for liver toxicity in animals, at the same time you're testing in all the other organs.
So they're gonna still be doing those animal studies, but the reality is that very, very frequently they get completely different results in dogs and rats and human cells in vitro, and they don't know what to do and they kind of wing it, and that's why there's lots of failures. Okay? So the context of use would be to use this human liver chip, particularly in those situations, to say do we go/no-go? And these are huge, expensive decisions for these companies.
CHAKRABARTI: Okay. So many more questions. We're running outta time here, so I'm gonna go as rapidly as I can, Dr. Ingber.
You mentioned expense. Now, Marty Makary at FDA and the NIH person that we heard earlier, everyone's talking about that ideally, these new technologies could actually — well, could potentially make drug development cheaper. Which then, those cost savings would ideally be passed on to patients in this country.
But what I'm also hearing at the same time is development of very, very sophisticated new technologies. And those technologies have to be getting patented. Right? So then you'd be licensing those technologies to the Mercks of the world. I actually see the potential for things becoming more expensive.
INGBER: Well, I'll give you two quick examples. One, the liver chip paper had an economic analysis that basically estimated that the pharmaceutical industry would save $2 to $3 billion a year by preventing late stage failures just from that one test. And if you did that for all the organs, it'd be like $27 billion a year.
The second example is that the company Moderna that developed the COVID vaccine — and they've presented this publicly, so I can say this, they've allowed us to use these slides — they have been using in-house the human liver chip instead of non-human primates to select which lipid nanoparticle's the delivery vehicle for vaccines and their mRNA drugs. Which ones could be toxic, which ones could be safe?
They were using non-human primates. Non-human primates are incredibly expensive, like $50,000, $60,000 an animal, besides the ethical issues. They basically can do the same amount of tests in about one-tenth the time and one-tenth the cost.
"They basically can do the same amount of tests in about one-tenth the time and one-tenth the cost."
CHAKRABARTI: I see.
INGBER: And the chips are very expensive in the early stages because it's a young field, but they will decrease in cost due to economies of scale over time.I think there would be a major savings. Animal studies are expensive. Very expensive.
CHAKRABARTI: Mm-hmm. And then you also, of course, mentioned the ethics, which are underlying everything, all issues for animal testing.
But you quickly went over a point, I just wanna emphasize this, that the idea is with these new technologies, there could potentially be fewer failures as you've called them --
INGBER: Late-stage failure, which are huge costs.
CHAKRABARTI: So drugs that end up going through the whole process, but not getting approved or not working for some reason.
INGBER: Which are most. Most drugs fail.
CHAKRABARTI: So by reducing that number, that should have a cost savings overall.
INGBER: Huge. I think the biggest game changer. Right now big companies will spend, you know, hundreds of millions on the drug development, tens of millions in a big clinical trial almost always fail. And then they go back and see is there a genetic subpopulation very similar that responded better? And they'll do a small trial, get approved for a narrow application.
You could flip it on the head with stem cells, patient-derived cells, organoids, organs-on-chips. Select a small group of patients that are very similar. Test the drugs for efficacy, test for toxicity. Use them for a small trial — faster, cheaper, more likelihood to succeed. It would be a total game changer, I think.
CHAKRABARTI: It would be a game changer for the companies. I will let reality settle in to see whether those companies actually pass the savings on to patients. Right? I'm not gonna ask you to answer that — or do you wanna answer that question? Because I think --
INGBER: No, I mean that's beyond our knowledge base.
CHAKRABARTI: Yeah. So I always listen skeptically to lawmakers when they're like, it will make it cheaper for patients. Well --
INGBER: But if one company does it, they will all do it. And if one company does it and starts charging less, that may push things down. That would be the hope.
CHAKRABARTI: Okay. Well, if any CEO's listening to this, I invite you to be the first company that does that.
Okay. We've got about five minutes left, Dr. Ingber. We could talk about the details and the technical details of organ on a chip, AI, et cetera, for hours. But I mean, come on. You and I are having this conversation like saying "Hooray, FDA, for finally announcing that they'll accept these alternative testing models" at the same time that FDA, NIH are being gutted by the Trump administration, that funding for research period is being wiped off the board.
I mean, it's impossible to, to talk about this in only rosy terms, when that is the other reality of, I mean, labs like yours, labs like Dr. Tam's. So talk to me about the impact that these politics and the funding cuts are having on this very area of research.
INGBER: Well, I mean, I'm at Harvard. So, you know, I got two of the first stop work orders and they both were on organ chip-related work.
But more importantly, the government's cutting funding across the entire nation. NIH, NSF, all, every university's getting hit. So we have — and then there's a proposed 40% cut in the next budget. So, everything's gonna slow. But more importantly, we're losing our young people.
"We've basically lost a generation ... of scientists in America because it's too much uncertainty."
And most of them are foreign students with visas because we attract the best and brightest who usually stay here, build companies, build the economy. And remember, the economy is driven by technologies and science drives technology. So I think this is gonna have a huge negative impact on the economy.
But in this area, it's gonna be hard. They're supporting this sort of work and alternatives, but whether you're gonna see funding there, I just don't know.
CHAKRABARTI: I want to hear this again. You received two stop work orders for organ on a chip related research.
INGBER: Absolutely.
CHAKRABARTI: What was that research?
INGBER: One of them was from BARDA and it was using chips to make models of human lung intestine, bone marrow and lymph node and to look at the effects of gamma radiation, to model radiation injury.
And then we're using AI and various sophisticated chemical screens and genetic screens to develop countermeasure drugs that can protect you from radiation, for example, in the case of a nuclear disaster or war and so forth, you know, a nuclear war.
And also for the other one came from NASA and we were basically developing chips with cells from the Artemis II astronauts who are going to the moon and these chips were gonna go up there alongside them to look at the effects of both microgravity and radiation, because you're not gonna get to Mars unless you have countermeasures against radiation.
And the idea was that you're only about four astronauts on a mission. But if we can prove that this worked, you could do many chips on these missions and begin to develop countermeasure drugs.
CHAKRABARTI: So there's no work happening on those two right now?
INGBER: No. Those have stopped completely. Yeah.
CHAKRABARTI: Now, you know, the Trump administration says, well, the Harvard-specific cessation of funding is to combat antisemitism. Was your research antisemitic?
INGBER: Well, I'm Jewish, and God, no. I mean, you know. And the Wyss Institute is sort of a separate 501c3. We're in Boston, we're nowhere near — and also the antisemitic issues, events that happened were in 2023 in the fall, and the university leadership has changed based on that. They've made amends, they've made new policies. Is it perfect? No, but there's actually a legal process where a government can go and try to ask for specific changes.
This is pure — I said in another interview, it's pure punitive lunacy. It's retribution for something that we don't know what, why they're taking it out on science at a time where international competitiveness with places like China depends on science. I do not know.
CHAKRABARTI: It does feel to me that we are handing American primacy on the development of these life-changing technologies to China.
INGBER: I was in China in the fall, and they are putting something like a half a billion dollars into an institute, bringing the best and brightest from all over the country, one site, to develop human organ emulation systems, basically. I think it's human organ physiological emulation of — HOPE was what it was called. So, no, absolutely. They're moving full-force and we're giving it to them on a silver platter.
CHAKRABARTI: So on the one hand we have the Trump administration through FDA saying, oh, well we're gonna accept these other models for some drug testing. We're going to try to speed up reviews for drug applications. Great. But on the other hand, they're cutting off that research at the knees.
INGBER: Well, I, you know, reading the seed corn of science, right? I mean they, maybe for the next few years the drug companies will start using these, but the pipeline of the future, the better model, models that have, you know, bells and whistles that we need, like different types of sensors and real-time analysis and AI-integrated, that's gonna slow down.
CHAKRABARTI: Well, Dr. Donald Ingber, founding Director of the Wyss Institute for Biologically Inspired Engineering at Harvard University and also founder of Emulate. It's a leading manufacturer of organ on a chip systems.
By the way, we also did reach out to FDA directly for comment or if someone from FDA could join us. They did not respond to our request in time for the broadcast of this episode.
But Dr. Donald Ingber, it's been a great pleasure to have you. Thank you so much.
INGBER: Oh, my pleasure. Thank you.
The first draft of this transcript was created by Descript, an AI transcription tool. An On Point producer then thoroughly reviewed, corrected, and reformatted the transcript before publication. The use of this AI tool creates the capacity to provide these transcripts.
This program aired on June 4, 2025.

