Support WBUR
Commentary
'There is no before': Life in the emergency department, two years into the pandemic
My wife and I just watched “Station Eleven,” a miniseries about the imagined “after” of a modern-day flu pandemic. In the moments of longing for what life used to be like, we’ll say to each other, “There is no before.”
As director of the emergency room at St. Luke’s Hospital, a community hospital in New Bedford, Mass., it can feel like there’s no “before” in healthcare either, as we find ourselves in an “after” that’s unsustainable, as the pandemic rages — again.
This time two years ago, we were fully staffed, and our emergency department ran like a well-oiled machine. We would regularly see 300-plus patients in a day. When patients arrived by ambulance, we immediately got them into beds. Rarely were there more than 15 people in the waiting room, where the wait time was almost never longer than an hour or two. We could accommodate all hospital admissions, meaning a patient in the emergency department would have a bed in the hospital within four hours, more often within the hour. But that was before.
Now, when I begin my shifts and check in with my charge nurse, I take in all of the yellow highlights on the schedule — the empty nursing and tech shifts we are desperately trying to fill. Over the past two years, I have seen dozens of these colleagues leave our ranks. The reasons are multi-faceted: burnout, better pay, easier work environment, different career options, family needs and illness being some of them. Currently, we have a 32% vacancy rate for nursing and an almost 40% vacancy rate for our techs and secretaries.
Our hospital capacity is graded by colors, with red being the most dangerous level of hospital crowding. I’ve worked at St. Luke’s for 10 years and, pre-COVID, could count the number of times we went into code red on one hand. As I write this, we have been in code red for 59 days straight.
I’ve worked at St. Luke’s for 10 years and, pre-COVID, could count the number of times we went into code red on one hand. As I write this, we have been in code red for 59 days straight.
Because of the staffing shortage, it’s commonplace to begin a shift as I did last week, with 36 people in the waiting room. Just a few days ago it was 59. I’ve seen wait times as high as 15 hours. And we see a mix of everything: COVID symptoms, non-COVID concerns and many patients with both.
We have 60 separate rooms in our emergency department. At the end of last week, we had 62 “boarders” — those are patients who are already admitted to the hospital based on the emergency department’s evaluation, and awaiting a bed. Some wait for 48 hours. You read that right.
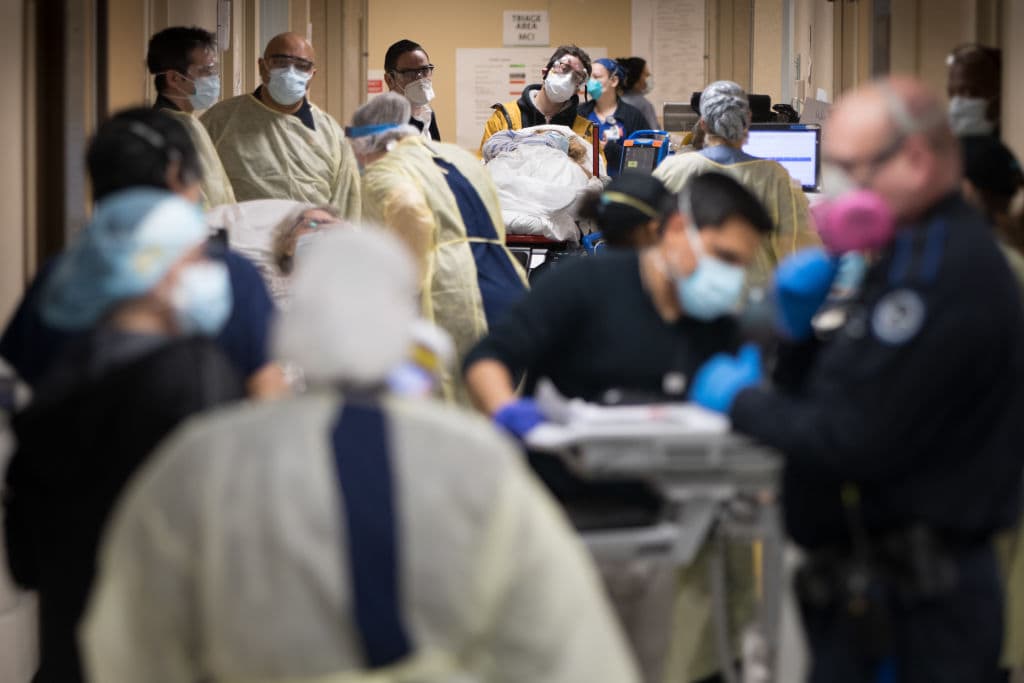
To accommodate those still waiting and needing care, we pack the hallways. We used to think we couldn’t handle more than 10 patients, maybe 15, in the hall. Now we regularly have more than 25.
Let me be clear that in the absence of adequate staffing and in the face of immeasurable burnout, we are bringing our hustle. We are seeing patients in the waiting room, in triage; we’re having doctors see patients with no nurse, so that the nurses we have aren’t stretched between an impossible number of patients. We’re using paramedics and putting the National Guard soldiers assigned to us to task.
The hospital has also re-deployed staff from other areas to help, especially now that elective surgery has been shut down again. We have anesthesiologists volunteering with their nurse anesthetists, starting IVs and drawing blood out in triage, and we have folks from the hospital’s communications and marketing teams volunteering to transport patients. We’re constantly trying to innovate and keep everyone safe, while working with less and less.
But you can see where this is going. The literature warns of “error and adverse events” on the heels of emergency department crowding and boarding. In short: things that are hard, get much harder. This is, to use Carl Zimmer’s analogy, like being clobbered by category 3 hurricane after a category 5 hurricane.
So, what does it look like to me? It’s a frail elderly gentleman about to fall as he climbs out of his hallway stretcher, caught by a passing radiology tech who happens to walk by at the right time. He’s sandwiched next to an intoxicated and incontinent woman screaming profanities, and a trauma patient wearing a neck collar with a head laceration slowly bleeding down his face. They will all have to wait. I see this on every shift.
[W]e have folks from the hospital’s communications and marketing teams volunteering to transport patients.
It’s answering a call about a patient transfer, just as you hear an overhead page for a trauma arrival, immediately followed by a stat page to go to a room for a medical code. (Code is doctor-speak for somebody’s heart stopped and needs to be revived.) Because four nurses and two techs at minimum are occupied by the trauma and the coding patient, the other 30 patients they share have to wait.
It’s watching our environmental services staff literally breaking a sweat trying to quickly but thoroughly clean a room, at the same time a patient down the hall screams at a doctor after being restrained by our safety officers, for spitting at and taking a swing at his nurse. It’s later, seeing the social worker have an earnest conversation with that same patient, trying to help get him into detox.
It’s coding a patient and not being able to find gel for the ultrasound machine because there aren’t enough techs to adequately stock the rooms. The only two techs on this side of the emergency department are taking turns doing chest compressions for a young man who stopped breathing after an opioid overdose.
It’s seeing three ambulance stretchers lined up in the hall because the charge nurse can’t receive them yet — he's helping wheel a patient back from the waiting room who just had a seizure. On one of the stretchers is a kid who’s seeing all of this too, until someone can whisk him away to the pediatric section.
For those of us who are still here, the camaraderie and dedication that brought many of us to this field carry over from before … for now.
Despite all of this — and it’s a lot — it’s also getting back to my computer just as the physical therapist places a Hershey kiss on the desk next to me, making me laugh through my N95 mask. For those of us who are still here, the camaraderie and dedication that brought many of us to this field carry over from before … for now.
We can and should talk about how to solve our current crisis, how to rebuild the workforce and sustainably engineer capacity into our healthcare system, how to incentivize young people into the field, what fair and equitable compensation looks like, how to prevent error, improve quality, how to do better. But right now? We’re just getting through each day.
Through all the cacophony of sound, movement, facts and feelings, I am immeasurably proud of our team — our salty crew — and the grit and grace and humor they bring just by continuing to show up every day.
It isn’t just this surge, or even the pandemic, that we need to be talking about. It’s the “after,” when the tsunami recedes and what’s left in its wake is a depleted patchwork of people trying their best to care for those who will continue to need it.
